This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
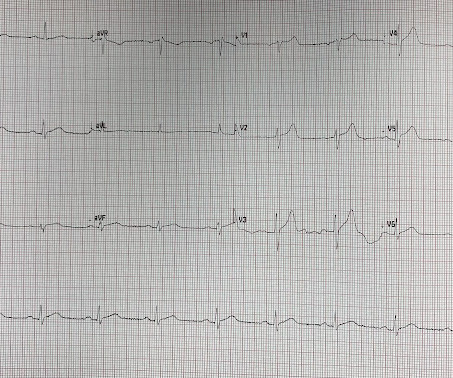
This ECG was recorded on arrival in the ED: Here is the interpretation of the conventional algorithm (Veritas): SINUS BRADYCARDIA ST ELEVATION, PROBABLY EARLY REPOLARIZATION [ST ELEVATION WITH NORMALLY INFLECTED T-WAVE] BORDERLINE ECG What do you think? Regional wall motion abnormality-apical septum and inferior wall.
He said that his pain does not feel like his previous episode of pericarditis, and is not related to meals. He denied chestpain, shortness of breath, nausea, fever, chills, rashes, cough, and leg pain. Does subsegmental pulmonary embolism matter? The ST/T ratio in V6, however, is slightly greater.
His first electrocardiogram ( ECG) is given below: --Sinus bradycardia. As his pain was very severe, emergency physicians concerned of aortic dissection and ordered a thoracic CT scan. Bi-phasic scan showed no dissection or pulmonary embolism. As he seemed very agitated, fentanyl and diazepam were given.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Frequent or repetitive PACs ii.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. Third, a slow motion segment showing delayed, brisk filling of the PDA due to dislodgment of a thrombus from contrast injection and distal embolization.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content