This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The patient’s chestpain spontaneously resolved before he was evaluated and has a repeat ECG obtained at 22:12 obtained shown below. Soon afterward, the patient’s symptoms return along with lightheadedness, bradycardia, and hypotension. It is unclear if he received aspirin at triage. This ECG is more difficult.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Angiography revealed a 30% nonobstructive stenosis of the mid LAD.
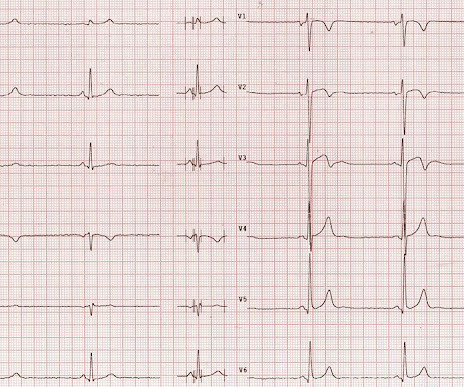
This ECG could easily be seen in an ED chestpain patient, and I have seen many) What do you think? Description Sinus bradycardia. Comment I (Smith) have seen many similar ECGs in ED chestpain patients. I have seen this innumerable times in chestpain patients in the Emergency Department.
Hopefully a repeat echocardiogram will be performed outpatient. ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. 1900: RBBB and LAFB are almost fully resolved.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chestpain. The computer called "Sinus Bradycardia" only (implying that everything else is normal. The overreading Cardiologist called it only "Sinus Bradycardia" with no other findings. There is zero ST Elevation.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chestpain: V5 and V6 sure look like a STEMI For this ECG and chestpain in the ED, the Cath lab activated. But the angiogram was clean.
However, an echocardiogram is a different test, also conducted for heart activity. If you experience any symptoms, such as chestpain, dizziness, unusual tiredness or fatigue, shortness of breath, or irregular heartbeat, your doctor would want you to go for an ECG test to find out the underlying cause.
The relationship between low RHR and CI has yet to be described.Purpose:We hypothesize that resting sinus bradycardia (low RHR) could be a predictor of chronotropic incompetence and reduced exercise capacity.Methods:The derivation cohort consists of 201 patients with normal Bruce protocol treadmill stress echocardiogram.
His medical history is unremarkable except a similar pain occurred 4-5 times in the previous 3 months with less intensity, short duration, unrelated to exertion. He visited an outpatient clinic for it and an echocardiogram and exercise stress test was normal. His first electrocardiogram ( ECG) is given below: --Sinus bradycardia.
5 years ago Similar Previous formal echocardiogram Inferior posterior with dyskinesis "Dyskinesis" is the technical echo term for LV aneurysm. The combination of absence of chestpain and history of LV aneurysm made it easy to assess that this patient does not have acute OMI. The patient ruled out by serial troponins.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. It was from a patient with chestpain: Note the obvious Brugada pattern. The Troponin I was cycled over time and was 0.353 followed by 0.296. This patient ruled out for MI.
The pneumothorax was expanded with a chest tube At 17 hours, another ECG was recorded: It is now much less dramatic and has the morphology of Type 2 Brugada The hs troponin I peaked at 6500 ng/L -- this strongly suggests myocardial contusion. An echocardiogram was done. Is there also Brugada? Right ventricular prominence.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Frequent or repetitive PACs ii.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content