This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundHypertrophic cardiomyopathy (HCM) is an autosomal dominant disorder characterized by asymmetric hypertrophy of the ventricles and the ventricular septum, leading to subsequent left ventricular outflow tract (LVOT) obstruction and diastolic dysfunction.
And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis.
During the night, while on telemetry, the patient became bradycardic, with periods of isorhythmic AV dissociation (nodal escape rhythm alternating with sinus bradycardia), and there were sporadic PVCs. The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia. Learning points: 1.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. The granulomatous inflammation affects the heart, causing an infiltrative cardiomyopathy The most common manifestations of cardiac sarcoidosis are atrioventricular (AV) block and ventricular tachyarrhythmias (VT).
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
They had a history of non-ischemic cardiomyopathy (EF 30%), as well as PCI with one stent. Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. I said I think there is a fixed stenosis in the LAD and the tachycardia and stress caused a type 2 STEMI.
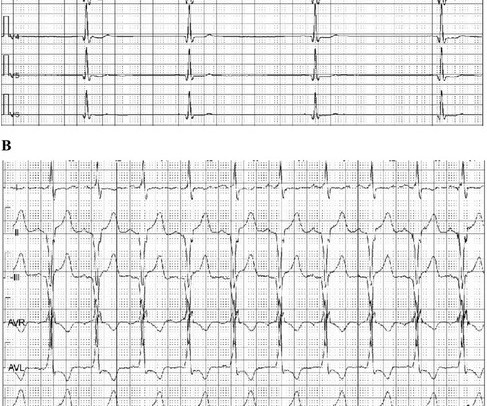
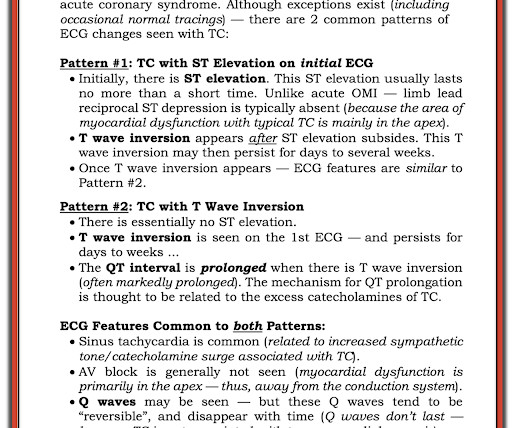
The patient was diagnosed with stress cardiomyopathy. Widespread T wave inversions and prolongation of the QT interval is not uncommon in Takotsubo cardiomyopathy. The QTc then gradually shortened over the course of several days as is usual for stress cardiomyopathy. Potassium was 4,8 mmol/l. ( ref 3,5-4,6 mmol/l ).
The deep learning algorithm helps segment the left ventricle predicting cardiomyopathy and ejection fraction. Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia.
A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. An ECG machine is able to detect other abnormalities of the heart as well, such as hypertrophic cardiomyopathy or overly thick heart muscles. Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat.
Other than tachycardia, Other than slight tachycardia, vitals were within normal limits (including oxygen saturation). As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. Were they right?
This ECG shows a sinus bradycardia with a normal conduction pattern (normal PR, normal QRS, and normal QTc), normal axis, normal R-wave progression, normal voltages. Hypothermia can also produce bradycardia and J waves, with a pseudo-STEMI pattern. There is marked sinus bradycardia. What do you think? As per Drs.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Repeat ECG was obtained immediately, just 24 minutes after the prior ECG: Given the context, my top differential diagnosis would be stress cardiomyopathy AKA takotsubo. Bradycardia and heart block are very common in RCA OMI.
There was never ventricular fibrillation (VF) or ventricular tachycardia (VT), no shockable rhythm. By ECG alone: it is suspicious for stress cardiomyopathy, or takotsubo, due to the diffuse ST Elevation: II, III, aVF AND I and aVL. Here is a similar case: Collapse, Ventricular Tachycardia, Cardioverted, Comatose on Arrival.
MY Thoughts on ECG #1: The rhythm is sinus bradycardia at a rate just under 60/minute. Figure-6: ECG Findings in Takotsubo Cardiomyopathy — adapted from Namgung in Clin Med Insights Cardiol ( See text ). There is sinus tachycardia at ~100/minute — with diffuse ST-T wave depression. No chamber enlargement.
Whenever I see PVCs with the morphology and axis seen in todays case I always look for signs of AC ( Arrhythmogenic Cardiomyopathy ). Arrhythmogenic cardiomyopathy often manifests with PVCs from the RV. The ECG in Figure-1 however, shows no signs of arrhythmogenic cardiomyopathy. Try a different kind of antiarrhythmic.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content