This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundHypertrophic cardiomyopathy (HCM) is an autosomal dominant disorder characterized by asymmetric hypertrophy of the ventricles and the ventricular septum, leading to subsequent left ventricular outflow tract (LVOT) obstruction and diastolic dysfunction.
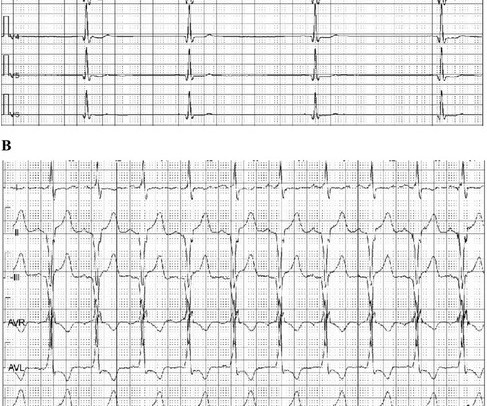
And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis.
Complete left bundle branch block (CLBBB)-like QRS morphology of right ventricular pacing at pacemaker implantation satisfying the American Heart Association/American College of Cardiology Foundation/Heart Rhythm Society criteria of CLBBB was associated with development of pacing induced cardiomyopathy.
The overall rhythm is chaotic — which is not necessarily unexpected given the history of an acutely ill 12-year with severe dilated cardiomyopathy on Echo. I’d guess the overall rhythm is sinus, perhaps with a wandering atrial pacemaker and very frequent ventricular ectopy with multiple couplets.
It turns out that she has hypertrophic cardiomyopathy. Here is the echo report for this visit (after the negative angiogram): Hypertrophic cardiomyopathy with asymmetric septal hypertrophy. There was a question in the record of hypertrophic cardiomyopathy. Regional wall motion abnormality-distal septum and apex.
need to be reminded the etiology of cardiomyopathy plays crucial role in determining the cause of LBBB. This fact by itself tell us what could be the true mechanism of LBBB in dilated cardiomyopathy. In selected patients with discrete proximal LBBB the pacemaker stimuli may breakthrough the block.
Enlargement of the left ventricular cavity, increased wall thickness and increased trabeculations in athlete’s heart will have to be differentiated from conditions like dilated cardiomyopathy, hypertrophic cardiomyopathy and isolated left ventricular non-compaction. Differentiating Athlete’s Heart From Cardiomyopathies – The Left Side.
Isoprenalin was discontinued, and a temporary transveous pacemaker was implanted. The patient stabilized following pacemaker placement. For example — bradycardia and AV conduction disturbances are not uncommon with Hyperkalemia , with these conduction disturbances most often resolving once serum K+ is corrected.
A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. An ECG machine is able to detect other abnormalities of the heart as well, such as hypertrophic cardiomyopathy or overly thick heart muscles. Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat.
He received a permanent pacemaker during the subsequent inpatient stay. plaque disruption), the T waves still manifest markings of a previous state of suboptimal coronary flow that resolved: Type II supply-demand mismatch in the setting of extreme bradycardia. Left bundle branch block-induced cardiomyopathy: Myth or reality?
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Repeat ECG was obtained immediately, just 24 minutes after the prior ECG: Given the context, my top differential diagnosis would be stress cardiomyopathy AKA takotsubo. Bradycardia and heart block are very common in RCA OMI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content