This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis.
The ECG does not show any definite signs of ischemia. I thought the complete lack of QTc prolongation and anatomic localization of ECG findings made Takotsubo cardiomyopathy unlikely. It is unclear if the patient was pain free at this time. Initial high sensitivity troponin I returned at 6ng/L (normal 0.20
During the night, while on telemetry, the patient became bradycardic, with periods of isorhythmic AV dissociation (nodal escape rhythm alternating with sinus bradycardia), and there were sporadic PVCs. Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. Echo revealed normalized function.
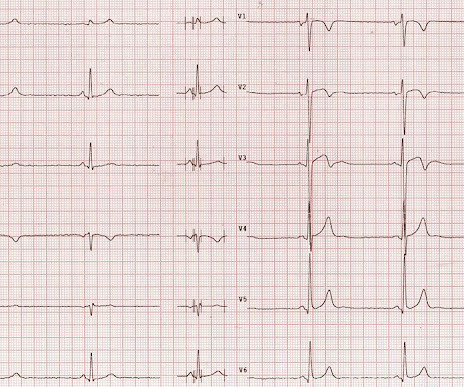
Description Sinus bradycardia. There is ST elevation in V2 and V3 There are inverted T-waves in V2 and V3 There are prominent U-waves in V2 and V3 Many responders were worried about ischemia or hypertrophic cardiomyopathy. This short QT at least makes ischemia all but impossible. There is high voltage.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. The fact that he has a cardiomyopathy argues for a more typical ventricular tachycardia, as does the absence of rSR' in lead V1. It is regular.
Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). The granulomatous inflammation affects the heart, causing an infiltrative cardiomyopathy The most common manifestations of cardiac sarcoidosis are atrioventricular (AV) block and ventricular tachyarrhythmias (VT).
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. LBBB is typically the result of preexisting hypertrophy, ischemic heart disease, or cardiomyopathy. 5] Isnard, R. & Pousset, F.
A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. Poor blood supply Ischemia, or inadequate blood supply to the heart, is an abnormality that can be detected in an ECG test. Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat.
Here was my answer: "Not ischemia. Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. This was texted to me in real time. The patient has acute chest pain. What do you think? Maybe HOCM or another form of LVH. I would not activate cath lab.
But when the clinical presentation is sepsis, one must entertain the possibility that the ST elevation is due to demand ischemia, or some other process, and exacerbated by tachycardia. It is prudent to treat the other conditions, get the heart rate controlled, and repeat the ECG.
This ECG shows a sinus bradycardia with a normal conduction pattern (normal PR, normal QRS, and normal QTc), normal axis, normal R-wave progression, normal voltages. Hypothermia can also produce bradycardia and J waves, with a pseudo-STEMI pattern. There is marked sinus bradycardia. What do you think? Pacing Clin Electrophysiol.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Repeat ECG was obtained immediately, just 24 minutes after the prior ECG: Given the context, my top differential diagnosis would be stress cardiomyopathy AKA takotsubo. Bradycardia and heart block are very common in RCA OMI.
By ECG alone: it is suspicious for stress cardiomyopathy, or takotsubo, due to the diffuse ST Elevation: II, III, aVF AND I and aVL. Subarachnoid hemorrhage causes extreme central catecholamine output, resulting in stress cardiomyopathy, just like takotsubo. This is unusual in acute OMI. she had severe pulmonary edema.
Whenever I see PVCs with the morphology and axis seen in todays case I always look for signs of AC ( Arrhythmogenic Cardiomyopathy ). Arrhythmogenic cardiomyopathy often manifests with PVCs from the RV. The ECG in Figure-1 however, shows no signs of arrhythmogenic cardiomyopathy. Therefore A different approach is needed.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content