This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis.
Complete left bundle branch block (CLBBB)-like QRS morphology of right ventricular pacing at pacemaker implantation satisfying the American Heart Association/American College of Cardiology Foundation/Heart Rhythm Society criteria of CLBBB was associated with development of pacing induced cardiomyopathy.
It turns out that she has hypertrophic cardiomyopathy. The diagnosis was a bit hard to find in the chart, and the echocardiogram did only stated "assymetric hypertrophy." Here is the echo report for this visit (after the negative angiogram): Hypertrophic cardiomyopathy with asymmetric septal hypertrophy.
Enlargement of the left ventricular cavity, increased wall thickness and increased trabeculations in athlete’s heart will have to be differentiated from conditions like dilated cardiomyopathy, hypertrophic cardiomyopathy and isolated left ventricular non-compaction. Differentiating Athlete’s Heart From Cardiomyopathies – The Left Side.
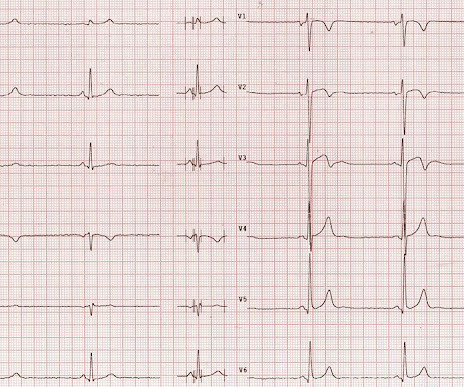
Description Sinus bradycardia. There is ST elevation in V2 and V3 There are inverted T-waves in V2 and V3 There are prominent U-waves in V2 and V3 Many responders were worried about ischemia or hypertrophic cardiomyopathy. (This ECG could easily be seen in an ED chest pain patient, and I have seen many) What do you think?
However, an echocardiogram is a different test, also conducted for heart activity. A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. Electrocardiogram, echocardiogram, and some other tests are done for patients with cardiac arrest. ECG and EKG refer to the same thing.
Whenever I see PVCs with the morphology and axis seen in todays case I always look for signs of AC ( Arrhythmogenic Cardiomyopathy ). Arrhythmogenic cardiomyopathy often manifests with PVCs from the RV. The ECG in Figure-1 however, shows no signs of arrhythmogenic cardiomyopathy. Try a different kind of antiarrhythmic.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content