This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundHypertrophic cardiomyopathy (HCM) is an autosomal dominant disorder characterized by asymmetric hypertrophy of the ventricles and the ventricular septum, leading to subsequent left ventricular outflow tract (LVOT) obstruction and diastolic dysfunction.
And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis.
I thought the complete lack of QTc prolongation and anatomic localization of ECG findings made Takotsubo cardiomyopathy unlikely. In fact, the ECG was described as normal, and without serial ECGs or prior ECGs for comparison it could be. Initial high sensitivity troponin I returned at 6ng/L (normal 0.20
During the night, while on telemetry, the patient became bradycardic, with periods of isorhythmic AV dissociation (nodal escape rhythm alternating with sinus bradycardia), and there were sporadic PVCs. There was hyperkinesis of the basal segments and findings were interpreted as typical of takotsubo cardiomyopathy. Learning points: 1.
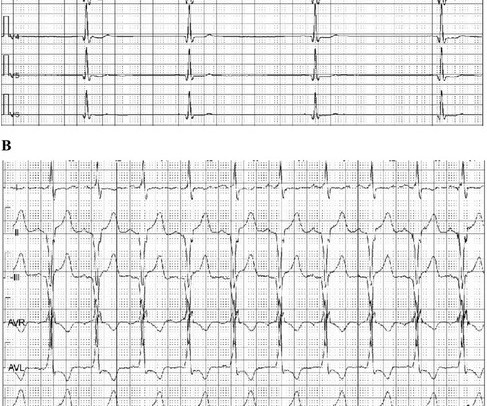
Complete left bundle branch block (CLBBB)-like QRS morphology of right ventricular pacing at pacemaker implantation satisfying the American Heart Association/American College of Cardiology Foundation/Heart Rhythm Society criteria of CLBBB was associated with development of pacing induced cardiomyopathy.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. The fact that he has a cardiomyopathy argues for a more typical ventricular tachycardia, as does the absence of rSR' in lead V1. It is regular.
It turns out that she has hypertrophic cardiomyopathy. Here is the echo report for this visit (after the negative angiogram): Hypertrophic cardiomyopathy with asymmetric septal hypertrophy. There was a question in the record of hypertrophic cardiomyopathy. Regional wall motion abnormality-distal septum and apex.
The overall rhythm is chaotic — which is not necessarily unexpected given the history of an acutely ill 12-year with severe dilated cardiomyopathy on Echo. There definitel are periods of bradycardia (so pacing may be needed for that). Hope this helps — :) ECG-3 — I see sinus bradycardia and arrhythmia.
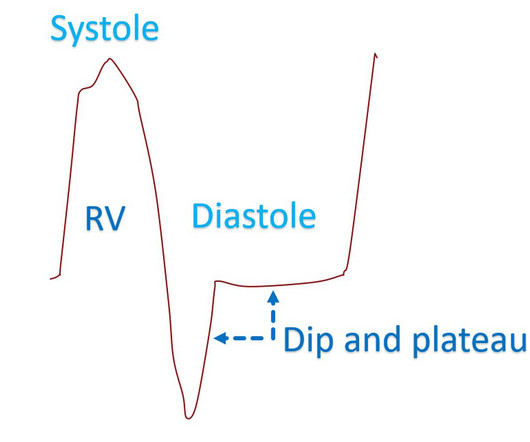
It is mentioned that square root sign can also occur in right right ventricular cardiomyopathy and severe bradycardia [1]. Reference Doshi S, Ramakrishnan S, Gupta SK. Invasive hemodynamics of constrictive pericarditis. Indian Heart J. 2015 Mar-Apr;67(2):175-82. doi: 10.1016/j.ihj.2015.04.011. 2015.04.011.
Enlargement of the left ventricular cavity, increased wall thickness and increased trabeculations in athlete’s heart will have to be differentiated from conditions like dilated cardiomyopathy, hypertrophic cardiomyopathy and isolated left ventricular non-compaction. Differentiating Athlete’s Heart From Cardiomyopathies – The Left Side.
need to be reminded the etiology of cardiomyopathy plays crucial role in determining the cause of LBBB. This fact by itself tell us what could be the true mechanism of LBBB in dilated cardiomyopathy. Myocardial LBBB (It is just LBBB morphology due to delayed conduction and not a true LBBB ) 4. No, it doesn’t correct it in all.
The patient was diagnosed with stress cardiomyopathy. Widespread T wave inversions and prolongation of the QT interval is not uncommon in Takotsubo cardiomyopathy. The QTc then gradually shortened over the course of several days as is usual for stress cardiomyopathy. Potassium was 4,8 mmol/l. ( ref 3,5-4,6 mmol/l ).
years during which 14 patients (18%) experienced VA requiring treatment ( n = 14) or syncope due to bradycardia ( n = 2). Survival analysis was performed to investigate the impact of LGE-CMR findings on survival free from adverse arrhythmic events. Patients were followed for 1.6 ± 1.5 95% confidence interval: [1.2–27],
They had a history of non-ischemic cardiomyopathy (EF 30%), as well as PCI with one stent. In most middle-aged patients with a history of cardiomyopathy, a WCT will usually be VT. Fragmentation suggests scarring (ie, from prior MI and/or cardiomyopathy ). Furthermore, while specific criteria (e.g.
The deep learning algorithm helps segment the left ventricle predicting cardiomyopathy and ejection fraction. Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia.
A triphasic left ventricular filling pattern with an additional mid diastolic wave, called T wave by some authors and L wave by others, can occur in situations of left ventricular diastolic dysfunction, especially in hypertrophic cardiomyopathy. Another video on this channel describes triphasic mitral flow in more detail.
Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. Smith's — in that despite the alarming ST-T wave changes, I did not think ECG #1 was the result of an acute event. QRS amplitude is dramatically increased in a number of leads.
Thus, there is a wall motion abnormality in the distribution of the LAD (not global apical dyskinesis, as in takostubo). This wall motion abnormality will almost certainly resolved with time (myocardial stunning).
The granulomatous inflammation affects the heart, causing an infiltrative cardiomyopathy The most common manifestations of cardiac sarcoidosis are atrioventricular (AV) block and ventricular tachyarrhythmias (VT). Lung involvement is the typical presentation. Cardiac sarcoidosis (CS) is seen in ~10% of patients with sarcoidosis.
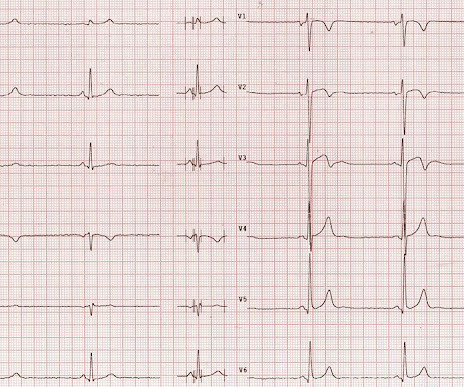
Description Sinus bradycardia. There is ST elevation in V2 and V3 There are inverted T-waves in V2 and V3 There are prominent U-waves in V2 and V3 Many responders were worried about ischemia or hypertrophic cardiomyopathy. (This ECG could easily be seen in an ED chest pain patient, and I have seen many) What do you think?
plaque disruption), the T waves still manifest markings of a previous state of suboptimal coronary flow that resolved: Type II supply-demand mismatch in the setting of extreme bradycardia. LBBB is typically the result of preexisting hypertrophy, ischemic heart disease, or cardiomyopathy. 5] Isnard, R. & Pousset, F. 6] Tabrizi, F.,
A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. An ECG machine is able to detect other abnormalities of the heart as well, such as hypertrophic cardiomyopathy or overly thick heart muscles. Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat.
As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. STD maximal in V1-V4 (in this case V3-V4) is in my opinion the single best way to identify posterior OMI on the anterior 12 lead ECG. Were they right?
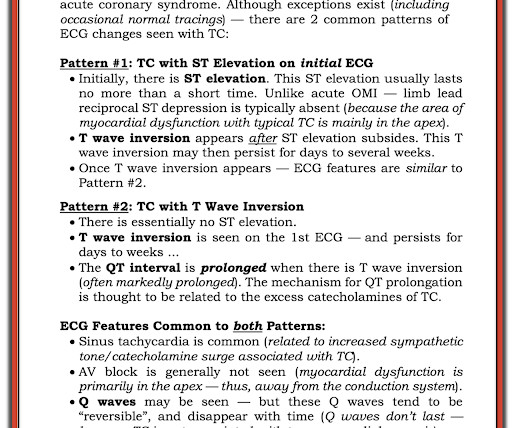
MY Thoughts on ECG #1: The rhythm is sinus bradycardia at a rate just under 60/minute. Figure-6: ECG Findings in Takotsubo Cardiomyopathy — adapted from Namgung in Clin Med Insights Cardiol ( See text ). This ECG picture is typical for Takotsubo Cardiomyopathy. Intervals ( PR, QRS, QTc ) and the axis are normal.
Background Variant transthyretin amyloidosis (ATTRv) is a hereditary multisystem disorder with clinical spectrum ranging from predominant cardiomyopathy to polyneuropathy. In the Irish population, the T60A mutation has been previously recognised as the most common genotype.
There is also STE in V1 which is diagnostic of right ventricular OMI in this situation , and partly explains the syncope and hypotension (along with the bradycardia). They recorded this ECG: Obvious inferior STEMI/OMI What else? The cath lab was activated by the medics.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Repeat ECG was obtained immediately, just 24 minutes after the prior ECG: Given the context, my top differential diagnosis would be stress cardiomyopathy AKA takotsubo. Bradycardia and heart block are very common in RCA OMI.
By ECG alone: it is suspicious for stress cardiomyopathy, or takotsubo, due to the diffuse ST Elevation: II, III, aVF AND I and aVL. Subarachnoid hemorrhage causes extreme central catecholamine output, resulting in stress cardiomyopathy, just like takotsubo. This is unusual in acute OMI. she had severe pulmonary edema.
Whenever I see PVCs with the morphology and axis seen in todays case I always look for signs of AC ( Arrhythmogenic Cardiomyopathy ). Arrhythmogenic cardiomyopathy often manifests with PVCs from the RV. The ECG in Figure-1 however, shows no signs of arrhythmogenic cardiomyopathy. Try a different kind of antiarrhythmic.
This ECG shows a sinus bradycardia with a normal conduction pattern (normal PR, normal QRS, and normal QTc), normal axis, normal R-wave progression, normal voltages. Hypothermia can also produce bradycardia and J waves, with a pseudo-STEMI pattern. There is marked sinus bradycardia. What do you think? As per Drs.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content