This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This can include our hearts, which may develop conditions like bradycardia or a slow heart rate. What Is Bradycardia ? Are you wondering “ What is bradycardia ?” Bradycardia is a condition in which the heart’s rhythm is too slow. Medications – Certain medications can slow down the heart rate as a side effect.
What happens to PR Interval in sinus Bradycardia ? Depends on the cause of Sinus bradycardia Answer When cardiac cycle slows down, every interval must get prolonged. Normally PR doesn,t stretch that far in isolated benign sinus bradycardia. The commonest cause of sinus bradycardia is due to increased vagal tone.
The patient was grimacing and agitated, presented with bradycardia at 40 beats per minute, and was mottled and cold. The patient was in a comatose state, the Glasgow Coma Scale Score was 8 (E2, V2, M4), with no localising neurological findings. The patient had last been seen well the previous day.
How do we figure out when bradycardia is due to a medical illness and when it is a primary cardiac problem? The post Ep 154: 4-Step Approach to Bradycardia and Bradydysrhythmias appeared first on Emergency Medicine Cases. What are some key ECG patterns that are sometimes missed by ED docs that can have devastating consequences?
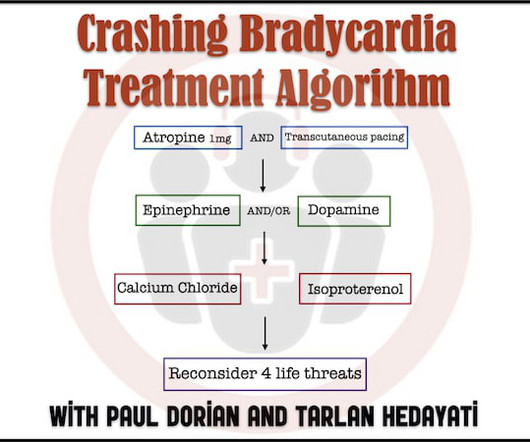
In Part 1 of our 2-part series on bradycardia and bradydysrhythmias we discussed a practical approach with electrophysiologist Paul Dorian and EM doc Tarlan Hedayati. How is the treatment of bradycardia different in the patient with hypothermia? In this, part 2, we discuss details of treatment. Cardiac ischemia? Myxedema coma?
BackgroundThere have been few instances of symptomatic bradycardia-arrhythmia in the context of area postrema syndrome (APS), and some of them have been implanted permanent pacemakers. A total of 21 cases were identified in the final analysis (including our case). The average age was 51 years old and female patients accounted for 38.1%.
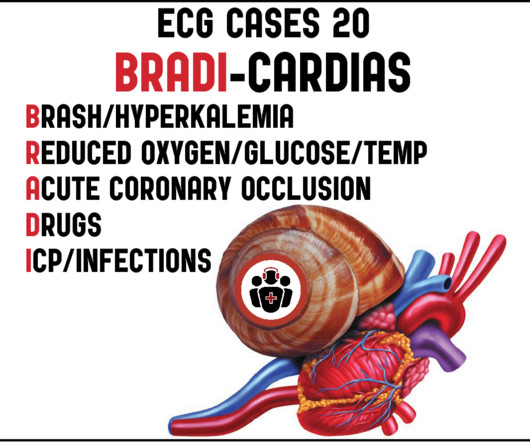
In this ECG Cases we review 10 patients who presented with bradycardia, introduce an approach to reversible causes using the BRADI mnemonic and guide you through how to use the ECG to guide management. The post ECG Cases 20 – Approach to Bradycardia and the BRADI Mnemonic appeared first on Emergency Medicine Cases.
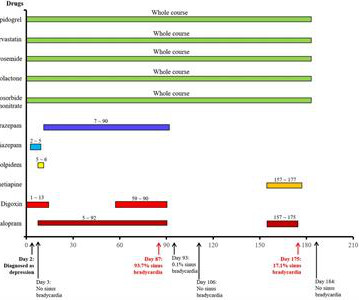
Here, a rare repeated sinus bradycardia event due to escitalopram is first reported. She began to take escitalopram and lorazepam due to depression, but sinus bradycardia (93.7% Escitalopram was deemed to be a highly possible cause of sinus bradycardia according to its Naranjo's Algorithm score.
See our other countless hyperkalemia cases below: General hyperkalemia cases: A 50s year old man with lightheadedness and bradycardia Patient with Dyspnea. A woman with near-syncope, bradycardia, and hypotension What happens if you do not recognize this ECG instantly? Also: How did this happen? Is this just right bundle branch block?
Men who perform well in the cross-country ski race Vasaloppet are at increased risk of having abnormally low heart rates and pacemakers later in life. However, the researchers behind the study did not uncover any link to increased mortality, rather the opposite—the skiers lived longer than the general population.
Bradycardia-dependent block is characterized by slowed or blocked conduction through His-Purkinje (HPS) fibers. We describe a case of bradycardia-dependent block after transcatheter aortic valve replacement (TAVR). A proposed mechanism is the diseased HPS develops spontaneous depolarization during phase 4 of the action potential.
Electrocardiogram (ECG) and telemetry revealed junctional bradycardia with heart rate in 30s and sinus pauses (5-7 seconds). He was admitted for further workup of bradycardia. His home medications included metoprolol succinate 25mg daily which was held given bradycardia. Initial laboratory analysis was unremarkable.
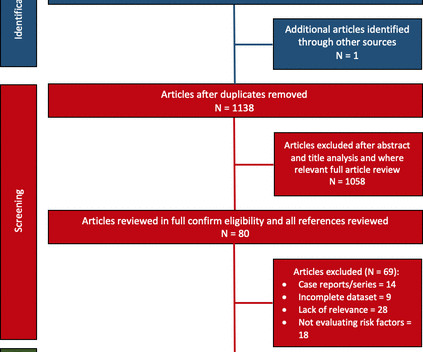
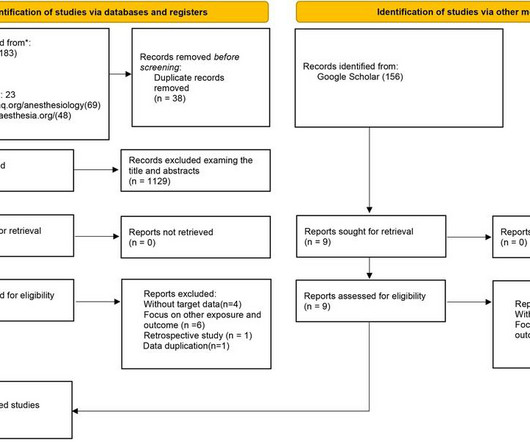
Objective We conducted a systematic review evaluating AF burden and bradycardia requiring permanent pacemaker (PPM) implantation and report any predictive risk factors identified. Study outcomes included AF or bradycardia requiring therapy. Databases included Embase, Medline, PubMed, Web of Science, CINAHL and Cochrane.
(MedPage Today) -- BOSTON -- A leadless pacemaker reliably communicated with a subcutaneous implantable cardioverter-defibrillator (S-ICD) to deliver anti-tachycardia (ATP) and bradycardia pacing, the MODULAR ATP study showed. In terms of safety.
Wireless implantable cardioverter-defibrillators (ICDs) eliminate the lead-related complications that come with a wired ICD, but they are unsuitable for patients with ventricular tachycardia, when the heart beats too quickly, or bradycardia, when the resting heart rate is seen as low.
We present a case series of two young patients with obesity-related comorbidities necessitating sleeve gastrectomy which provoked symptomatic sinus bradycardia. While weight loss following bariatric surgery often yields resolution of comorbidities related to obesity, it also presents unanticipated changes in underlying physiology.
It was never compared to other methods of dyssynchrony assessment in bradycardia patients. Ultra-high-frequency ECG (UHF-ECG) is a non-invasive tool visualizing the ventricular activation sequence.
Let's analyze the ECG. It comes from a pacemaker patient whose pacemaker was briefly switched to VVI at 30 bpm due to a stimulation threshold test. The first 3 beats show a sinus rhythm with a frequency of approx. This is followed by a premature ventricular contraction (PVC).
Her vital signs were within normal limits except for bradycardia at 55 bpm. It is probably sinus bradycardia with very small/depressed P-waves and prolonged PR interval. P EARL # 4 In my opinion, it is not worth wasting time trying to figure out the specific rhythm diagnosis of a bradycardia when there is hyperkalemia.
Resuscitation was initiated and this ECG was obtained: Likely AFib (irregularly irregular) with bradycardia. In addition to marked bradycardia — could there be high-grade AV block? On arrival in the ED, she was profoundly hypotensive, nearly obtunded, and bradycardic.
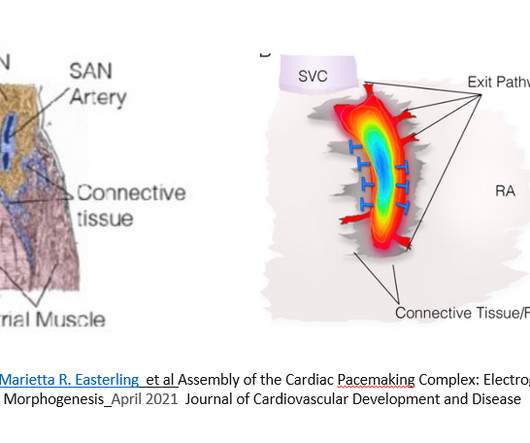
Using ECG recording and deductive reasoning, our teachers and predecessors classified the bradycardias and tachycardias and proposed many mechanisms, subsequently proven to be correct. Notwithstanding many insightful observations, the electrocardiogram (ECG) arguably ignited the big bang in our understanding of cardiac arrhythmias.
As the most common cause of syncope, vasovagal syncope (VVS) is the result of cerebral hypoperfusion caused by sudden-onset bradycardia and mediated by parasympathetic overdrive.1 1 VVS is generally categorized into three types: cardioinhibitory, vasodepressive and mixed type.
For instance, if there were inappropriate sinus bradycardia at less than 60 bpm, the atrial pacer would take over if it is programmed to wait 1 second before firing. The atrial lead would pace if, after a programmed period of time, it did not sense an atrial beat (usually 1 second, corresponding to a rate of 60).
Both of these features make inferior + RV MI by far the most likely ( Pseudoanteroseptal MI is another name for this ) There is also sinus bradycardia and t he patient is in shock with hypotension. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
Methods Consecutive patients with bradycardia indicated for pacing from 2016 to 2022 were prospectively followed for the clinical endpoints of heart failure (HF)-hospitalizations and all-cause mortality at 2 years. CSP should be preferred over VSP or RVP during pacing for bradycardia.
Among them, bradycardia and pause detection could be erroneous during sleep as the heart rate may slow down significantly leading to potential inappropriate diagnosis. Insertable cardiac monitors (ICMs) are used widely for long term monitoring and diagnosis of various cardiac arrhythmia.
Crew notifies the received ED of an incoming post-arrest patient and notes a sinus bradycardia on their monitor, as seen in Figure 2. Figure 2 : This rhythm shows a sinus bradycardia at a rate between 30 and 40bpm. The crew immediately initiated TCP at a rate of 70bpm and slowly increased the current, as shown in Figure 3.
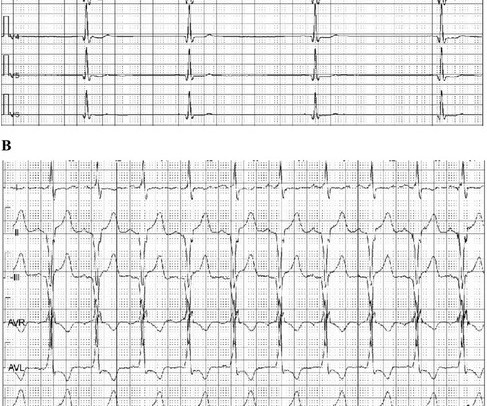
The ECG shows an example of a patient with bradycardia/tachycardia syndrome. Patients with bradycardia/tachycardia syndrome usually require a heart pacemaker to prevent the heart rate from becoming too slow. Initially, a sinus rhythm with a heart rate of approx. 70 bpm is seen. 120 bpm here). 120 bpm here).
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. As described above by Dr. Smith Pacing in today's case is an effective intervention as doing so prevents the bradycardia and pauses that are likely to precipitate additional episodes of Torsades de Pointes. (
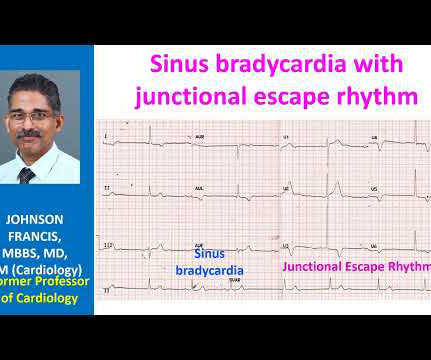
There’s competing sinus bradycardia and junctional rhythm, with otherwise normal conduction, borderline right axis, normal R wave progression and voltages. Significant bradycardia ( rate in the 40s/minute ) — is present throughout. What do you think? It’s unclear if the paramedic ECGs were seen or missed in the ED.
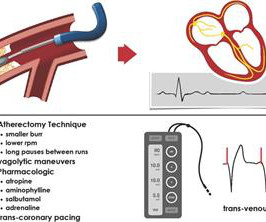
Background Rotational atherectomy (RA) during percutaneous coronary intervention may cause transient bradycardia or a higher-degree heart block. Traditionally, some operators use prophylactic transvenous pacing wire (TPW) to avoid haemodynamic complications associated with bradycardia.
Does prolonged, high-intensity endurance training increase the risk of bradycardia requiring pacemaker implantation and ultimately the long-term mortality risk?
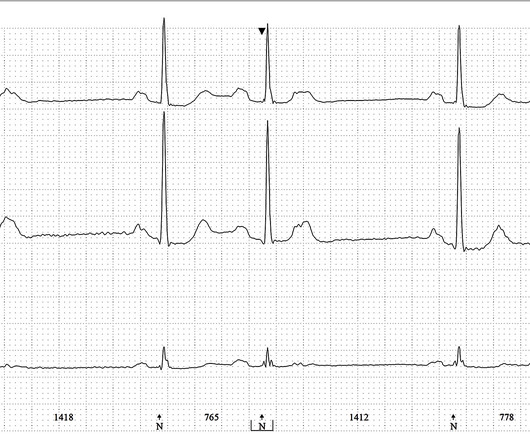
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
The primary outcome was ventricular arrhythmias, the secondary outcomes were bradycardia and atrial fibrillation (AF).ResultsOur 0.66], but increased the risk of in-hospital bradycardia (OR 2.88, 95% CI 1.02–8.17) 0.66], but increased the risk of in-hospital bradycardia (OR 2.88, 95% CI 1.02–8.17) 8.17) compared with propofol.
A common cause of pauses and bradycardia are non-conducted PACs, which generally do not require treatment. Therefore, it is important to differentiate between pauses or bradycardia that require treatment.
Left bundle branch block (LBBB) is a frequent complication of transcatheter aortic valve implantation (TAVI) and was shown to predict advanced atrio-ventricular block and pacemaker implantation (PI).1,2 1,2 Previous studies focused on persistent TAVI-induced LBBB. There are limited data on TAVI-related intermittent LBBB.
In-hospital cardiac arrest (IHCA) is a major healthcare problem with a high mortality rate. With continuous telemetry monitoring, heart rate trends could be used to predict IHCA events.
Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). Finally — If today's patient does not have significant underlying coronary disease — then her bradycardia with AV block may be the result of SSS ( S ick S inus S yndrome ).
The first two beats are sinus node beats, there is a sinus bradycardia with approx. After this, the sinus bradycardia is re-established. We see the limb leads + V1/V2. Then there is a sinus arrest with a pause of 3000 ms, which is interrupted by a junctional escape beat.
Altered Mental Status, Bradycardia == MY Comment , by K EN G RAUER, MD ( 2/2 /2024 ): == Dr. Meyers began today’s case with the clinical challenge of asking you to identify the underlying cause of ECG #2. -- Read this ECG -- Osborn Waves and Hypothermia (this is the "Figure" above) What does LBBB look like in severe hypothermia?
There is no P wave in front of each QRS, so this is not sinus bradycardia. If the patient is showing signs of poor perfusion, we would stop here and prepare to increase the rate with a temporary pacemaker (transvenous or transcutaneous). Why is the rate so slow?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content