This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Catheter ablation (CA) for symptomatic atrial fibrillation (AF) offers the best outcomes for patients. Despite the benefits of CA, a significant proportion of patients suffer a recurrence; hence, there is scope to potentially improve outcomes through technical innovations such as ablation index (AI) guidance during AF ablation.
In the light of increasing availability, the analyses of outcome-relevant predisposing characteristics are of growing importance. The primary outcome was defined as the survival of patients until they were discharged from the hospital, with a favourable neurological outcome [cerebral performance category (CPC) score of ≤2].
IntroductionRecent findings suggest that general anesthesia with endotracheal intubation (GA) in patients with acute ischemic stroke (AIS) due to large vessel occlusion (LVO) who receive mechanical thrombectomy (MT) is associated with similar outcomes to conscious sedation (CS). [1][2] 83 patients received GA and 159 patients received CS.
Patients with more severe obesity were more likely to have responder characteristics for atrial shunt therapy (fewer pacemakers and lower exercise pulmonary vascular resistance [PVR]). of patients had BMI ≥30 kg/m 2. Strain measurements in all four chambers were maintained as BMI increased. Overall, 60.9%
Obesity is associated with increased cardiovascular risk and adverse cardiac changes such as left ventricular hypertrophy (LVH) and in TOF higher body mass index (BMI) contributed to increase risk. Future larger and longitudinal studies are needed to determine if delayed repair in obese patients lead worse remodeling and outcomes.
The beneficial effects of finerenone in patients with heart failure (HF) and mildly reduced or preserved ejection fraction were consistent, regardless of a history of chronic obstructive pulmonary disease (COPD) status. BMI, body mass index; LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal pro-B-type natriuretic peptide.
Introduction:The demographics of patients with pulmonary arterial hypertension (PAH) is shifting towards older age, increased comorbidity burden, and an increase in the risk of left ventricular (LV) diastolic dysfunction. Survival analysis was performed (Outcome: PAH related-hospitalization or death). 2022 were included.
BMI, body mass index; CI, confidence interval; LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal pro-B-type natriuretic peptide. ABSTRACT Aim Chronic obstructive pulmonary disease (COPD) is common in heart failure with a mildly reduced or preserved ejection fraction (HFmrEF/HFpEF) and is associated with worse outcomes.
Association between body mass index (BMI) and clinical outcomes in PARADISE-MI. ( A ) Histogram for BMI (kg/m 2 ), ( B ) adverse events for BMI subgroups, and spline model curves for ( C ) the primary composite outcome and ( D ) cardiovascular (CV) death by BMI subgroups.
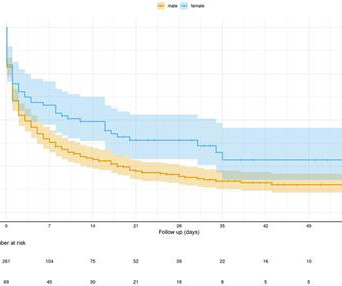
Background:Research into pulmonary hypertension (PH) reveals significant sex-based disparities in long-term survival rates. Notably, women, despite being more susceptible to PH, often experience better survival outcomes than men—a phenomenon possibly linked to the "estrogen paradox."
It is imperative to act swiftly when faced with such a medical emergency to ensure the best possible outcome. Keeping your healthy weight as per your BMI will lessen the risks. If the person receives timely treatment during this critical period, they can expect a near-complete recovery. Maintain a nutritious diet.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content