This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
These results highlight the potential of preventing increasing CKD burden and of preventing subsequent cardiovascular conditions, especially given current rates of obesity among adolescents.
a clinical-stage biopharmaceutical company focused on developing medicines to target hypertension, chronic kidneydisease (CKD) and other diseases, hasannounced that the U.S. Subjects will be at least 18 years old, with a BMI 27 kg/m 2 , and the trial will be conducted across approximately 40 sites.
BMI, body mass index; eGFR, estimated glomerular filtration rate; NYHA, New York Heart Association. Discontinuation occurred early and was more common in patients with advanced kidneydisease, hyperkalaemia, lack of follow-up in specialty care, more severe heart failure, comorbidities, and markers of sociodemographic frailty.
Physical activity (PA), body mass index (BMI), and blood glucose were associated with aTRH (all p-values<0.05), while diet, nicotine exposure, sleep, and blood lipids were not significantly associated with aTRH. Compared to subjects with low CVH, participants with moderate and high CVH exhibited lower risks of 47% and 76%, respectively.
17.4]) and was also more likely to have diabetes mellitus, hyperlipidemia, chronic lung disease, chronic kidneydisease, chronic liver disease, BMI ≥ 25, anemia, metastatic cancer, and atrial fibrillation. The hemophilia cohort was slightly older (63.2[16.8]
Propensity score-matched analysis (PSM) (1:1) was performed on age, gender, BMI, hypertension, diabetes mellitus, chronic kidneydisease, hemoglobin level, LDL level, left ventricular ejection fraction and various drugs including beta blockers, ACEi and ARBi. Both groups were followed for 12 months.
Propensity score-matched analysis (PSM) (1:1) was performed with matching for age, gender, race, BMI, hypertension, diabetes mellitus, chronic kidneydisease, hemoglobin level, low-density lipid (LDL) level, left ventricular ejection fraction, and various drugs including ACEi, ARBi, ARNI, beta-blockers, and diuretics.
Even in diabetics of normal weight (BMI<27), weight loss can reverse diabetes 2. If you are doing the appropriate aerobic and resistance training levels, you should be at the higher end (If you have serious kidneydisease, you should speak with your dietician). What should you eat to do this? Maintain, gain or lose weight?
There are significant data that show that if you have obesity, you have a high risk of developing coronary heart disease, heart failure, type 2 diabetes (T2D) or risk factors such as hypertension and dyslipidemia. [1] These individuals tend to have a better prognosis when compared to both individuals with normal weight (BMI of 18.5
Reliability of self-reported risk factors was high in overweight (F1 0.81) and diabetes (F1 0.71), moderate in hearing impairment (F1 0.59) and hypertension (F1 0.56) and low in hypercholesterolemia (F1 0.49) and kidneydisease (F1 0.25).
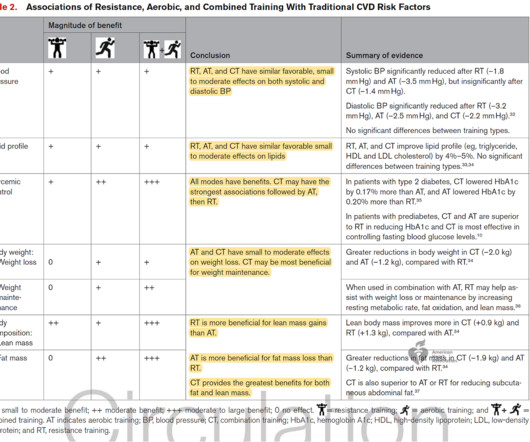
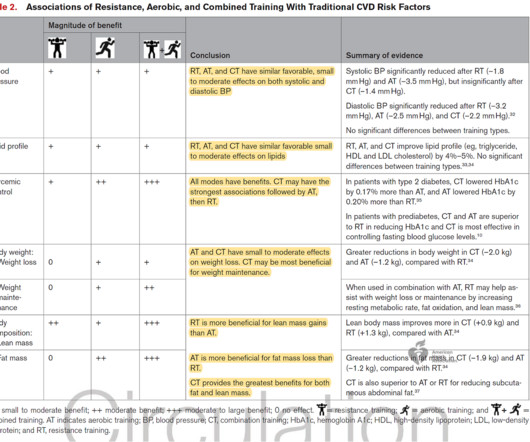
Of course, these benefits can also extend to individuals with a BMI in the normal range. For adults with overweight and obesity, resistance exercise increases lean body mass and reduces body fat percentage and fat mass — improving overall body composition. RT Prescription Resistance training need not be complicated to be effective.
Of course, these benefits can also extend to individuals with a BMI in the normal range. For adults with overweight and obesity, resistance exercise increases lean body mass and reduces body fat percentage and fat mass — improving overall body composition. RT Prescription Resistance training need not be complicated to be effective.
Asthma significantly increased the prevalence of stroke among participants aged 1844 years old, with a BMI 18.5029.99kg/m2, with low education levels, and with a PIR<1.00. Asthma also increased the prevalence of angina in females, non-Hispanic Blacks, participants aged 4559 years old, with a BMI30.00kg/m2, and with a PIR<1.00.
Pseudotime progression associated with higher HbA1c, BMI, and GBM, and lower insulin sensitivity and cortical oxidative metabolism.CONCLUSION These early structural and metabolic changes in T1D kidneys may precede clinical DKD.TRIAL REGISTRATION ClinicalTrials.gov NCT04074668.FUNDING
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content