This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Because CBF is not easy to measure, rises in heart rate or drops in bloodpressure are used as proxies for abnormal CBF. These result in diagnoses such as postural orthostatic tachycardia syndrome and orthostatic hypotension.
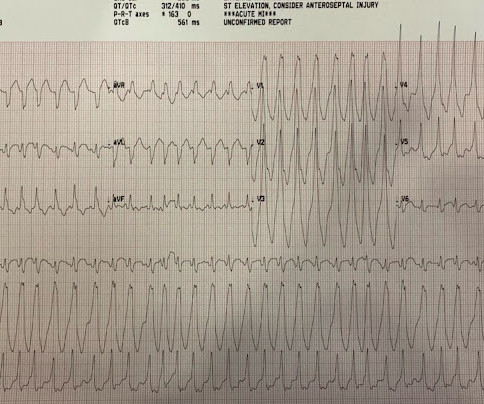
Bloodpressure was 117/80, pulse 161, Resp 45, SpO2 100 on oxygen. Here is the 12-lead ECG: Wide complex tachycardia What do you think? His pulse on the monitor suddenly went down to 140 and another 12-lead ECG was recorded: Sinus tachycardia at a rate of 143 There are peaked T-waves typical of hyperkalemia The K returned at 6.9
Then I always look to see if the initial deflection of the QRS has a lot of voltage change per change in time (seen in tachycardias that are initiated from above the ventricle because the propagate through fast conducting purkinje fiber. Tachycardia exaggerates ST Elevation in LBBB and Paced rhythm 5. Pacemaker mediated tachycardia!
The ECGs show a wide complex, irregularly irregular tachycardia. His bloodpressure was 118/96. At that time, he presented via EMS and had received magnesium and lidocaine prehospital for concerns of ventricular tachycardia. On arrival to the ED, he was noted to be in a wide complex tachycardia with a rate in the 240s.
Mentation and bloodpressure were normal. But it is not disorganized enough to be polymorphic ventricular tachycardia. Learning Points: Wide complex irregularly irregular tachycardias include PMVT, AF with WPW, and AF with aberrancy. See our other cases of AF with WPW: A young man with another episode of tachycardia.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
On the monitor patient had wide-complex tachycardia. Differential is ventricular tachycardia versus supraventricular tachycardia with aberrancy versus sinus tachycardia with a aberrancy. After the patient was stabilized with supportive care, the heart rate gradually slowed, confirming sinus tachycardia.
His examination was normal (with a bloodpressure of 120/70mmHg) except for tachycardia (Figure 1). A 64-year-old man presented with epigastric discomfort and palpitations after a festive meal. He reported taking no medications.
He presented to the Emergency Department with a bloodpressure of 111/66 and a pulse of 117. He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. He had this ECG recorded.
This is because stress causes an increase in cortisol – the primary stress hormone – leading to increases in bloodpressure , cholesterol, blood sugar and heart rate. Cold temperatures alone impact the body by causing the coronary arteries to constrict, bloodpressure to rise and the heart to work harder.
Bloodpressure was 180/80. Here was his initial ECG: Regular Wide Complex Tachycardia. Differential of Wide Complex Tachycardia (check out this post) -- Sinus with aberrancy -- Aberrancy can be due to toxins (wide complex from the many drugs which have sodium channel blocking effects and prolong the QRS) --SVT with aberrancy.
His previous echo one month prior shows the same thing: “consistent with old infarct in LAD vascular territory, with EF 45%” "I think there is something else causing his tachycardia which is exaggerating his EKG findings and mimicking an acute myocardial infarction." The patient spontaneously converted back to sinus tachycardia.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
They had already cardioverted at 120 J, then 200 J, which resulted in the following: Ventricular Tachycardia They then cardioverted at 200 J which r esulted in the same narrow complex rhythm shown above, at 185 beats per minute. This would treat both SVT or sinus tachycardia. I suggested esmolol if the heart rate did not improve.
Sometimes, head up tilt test, also known in short as HUTT, is also done for the evaluation of postural orthostatic tachycardia syndrome, POTS, a condition in which there is tachycardia on standing up, without a fall in bloodpressure. If syncope does not occur with 70 degrees tilt, it can be done at 80 degrees tilt.
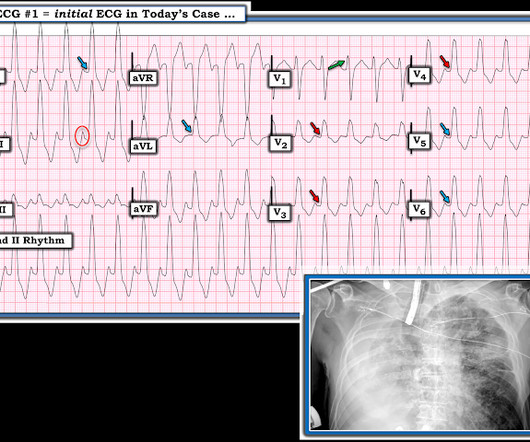
MY Thoughts on this CASE: Not being there — I am unaware of physical exam parameters ( bloodpressure, respiratory rate; oxygen saturation; heart and lung auscultation, etc. ). I see the following: There is sinus tachycardia ( upright P wave with fixed PR interval in lead II ) — at the rapid rate of ~130/minute.
Early detection of conditions like AFib, bradycardia, or tachycardia allows patients to address issues before they become critical. By understanding patterns in heart rate, bloodpressure, and oxygen levels, surgeons can tailor procedures to the individuals needs.
Dr Sanjay Gupta, a consultant cardiologist at York Hospital, is an expert in POTS, or postural tachycardia syndrome. The condition can leave sufferers debilitated, constantly exhausted, and sometimes unable even to walk.
Although sinus tachycardia is the most commonly encountered rhythmic disturbance, subsequent reports have highlighted other findings. She presented with presyncope and an initial bloodpressure of 77/63 mmHg. Echocardiography confirmed signs of right ventricular dysfunction.
On examination, the pulse rate was around 190 beats/min with a systolic bloodpressure of 80 mm Hg. ECG at presentation was suggestive of ventricular tachycardia (VT) ( figure 1 A ). Resuscitation with urgent cardioversion in view of haemodynamic instability with wide complex tachycardia was done.
BloodPressure Many medications used to treat congenital heart disease can affect bloodpressure levels. It’s crucial to monitor your bloodpressure regularly and report any significant changes to your healthcare provider so they can adjust the dosage of the medication accordingly.
On arrival in the emergency department, invasive bloodpressure was 35/15mmHg and the patient was in profound cardiogenic shock with severe confusion secondary to brain hypoperfusion. The arterial blood gas showed a lactic acidosis with a lactate level of 17mmol/L. PUSH THE LYTICS ! The below ECG (ECG #4) was recorded.
Blocking this enzyme helps relax blood vessels so there is a wider opening for better blood flow. This will lower bloodpressure, making it easier for the heart to pump. POTENTIAL SIDE EFFECTS: Potential adverse reactions include coughing, dizziness, kidney problems, and low bloodpressure.
Immediately after contrast injection into the LMCA, the patient had circulatory collapse, with a precipitous drop in bloodpressure. An Impella device was placed to maintain cardiac output and perfusion pressures. You can see Left Main and Proximal LAD obstruction, but with some flow, which is saving this patient's life.
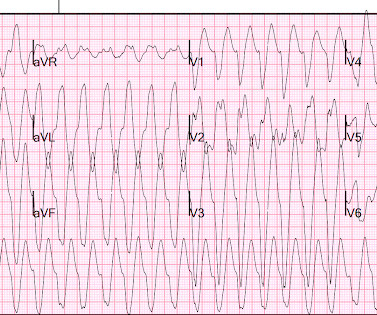
There is a regular, wide complex, (mostly) monomorphic tachycardia. The differential of wide, regular, monomorphic tachycardia is: VT or SVT with aberrancy, all +/- hyperkalemia (see diagrams below). Really wide tachycardia = VT or SVT with conduction abnormality + hyperkalemia, until proven otherwise.
Bloodpressure was normal (109/83). Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered.
Bloodpressure was 215/124 and HR 115 (on metoprolol). Here is his ED ECG: There is sinus tachycardia. The amount of ST elevation and depression is slightly less than on the ECG above, but there is also no tachycardia, which tends to exaggerate ST deviation.
Most Type 2 OMI are due to supply-demand O2 mismatch that do NOT involve a dynamic change in the coronanry artery: 1) decreased O2 supply from (a) low bloodpressure, especially in the presence of fixed coronary stenosis (b) hypoxia, (c) anemia (d) hemoglobinopathies such as CO poisoning or (e) oxidative phosphorylation problems (CN or HS) [(d) and (..)
The findings include sinus tachycardia, characteristic QRS morphology most diagnostic in V3 with a small R wave followed by a very large S wave with a convex upward ST segment morphology, ST segment strain morphology in the inferior and anterior leads leading to deep symmetric T-wave inversion. and tachycardia, 1.8. incomplete RBBB 1.7
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
The initial bloodpressure was 80/palp with a heart rate of 104, respirations 20, oxygen saturations of 94% and a finger stick blood glucose of 268. In addition, the patient received 750 mL of fluid resuscitation with transient improvement of bloodpressure.
The bloodpressure was 110/60. The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. It was not relieved by anything. The pain was not positional, pleuritic, or reproducible. He had no previous medical history. If it is MI, is it type 1 or type 2?
Prior ECG on file: Sinus tachycardia, imperfect baseline, otherwise unremarkable. Sinus tachycardia with unequivocal evidence of hyperkalemia, including widened QRS with "pulled apart" morphology (widened QRS) compared to baseline, as well as clearly peaked T-waves. Compartment pressures in the right calf were all 40-50 mmHg.
Given that there was such a high bloodpressure, it is possible that this is a type 2 MI (supply demand mismatch due to high oxygen demand when myocardium is pumping against such elevated bloodpressure.) Her initial cTnI returned at 0.25
2) Norepinephine to support BloodPressure. The RV is normally a low pressure chamber, and perfusion happens in both systole and diastole (unlike the LV, which only perfuses in diastole when the pump is not squeezing). The rhythm in ECG #1 is not Sinus Tachycardia — because there is no upright P wave in lead II.
On arrival in the ED, he was hypotensive with a systolic bloodpressure in the 70s. After initiating treatment for hyperkalemia, repeat ECG showed resolution of Brugada pattern: The ECG shows sinus tachycardia. A Very Wide Complex Tachycardia. Fluid resuscitation was initiated. What is the Rhythm? Use Lewis Leads!!
The cardiac monitor showed sinus rhythm but the automatic bloodpressure cuff was not reading. We arrived in the resuscitation bay and recorded a heart rate of 115 bpm and bloodpressure of 50/30 mm Hg. Why would she have such varying bloodpressure? She was discharged home in good condition.
pre-existing, stable atherosclerosis) amidst any state of global duress – to include hypertension, hypoxia, tachycardia, hypotension, sepsis, and GI bleed, for example. Although the bloodpressure resolved, his pain, however, did not. There may even be significant overlap between these factors.
He is placed on heparin drip, he will have IV beta-blocker and oral beta blocker for heart rate control and bloodpressure management. There is sinus tachycardia at 100-105/minute. "Discussed with the on-call cardiologist, there are currently no beds available at other facilities within the system, so he will be kept here.
Although the shock is no doubt partly a result of poor pump function, with low stroke volume, especially of the RV, it should be compensated for by tachycardia. This is particularly true of RV MI: LV coronary perfusion is dependent on diastolic pressure because the myocardial pressure is too high for perfusion during systole.
However, recent studies have observed that people below 40 are also experiencing heart attacks due to high bloodpressure, cholesterol, diabetes, smoking, obesity, a sedentary lifestyle, and social and mental stress. This indicates that restoring normal blood circulation as quickly as possible will result in less damage.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Any ED systolic bloodpressure less than 90 or greater than 180 mm Hg (+1) 4. h/o heart disease (+1) 3.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content