This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Infusions of potentially therapeutic cells derived from the heart are safe for people with pulmonary arterial hypertension, a form of high bloodpressure that occurs in the blood vessels of the lungs and typically affects middle-aged women, according to a new study.
A study conducted by scientists from Kaunas (Lithuania) universities has revealed the possibility of non-invasively reducing bloodpressure and speeding up gas exchange within the pulmonary system.
milla1cf Tue, 02/27/2024 - 17:29 February 27, 2024 — Aria CV, Inc , a developer of medical devices treating pulmonary hypertension, today announced the first patient was implanted with the Gen 2 Aria CV Pulmonary Hypertension System as part of the ASPIRE PH clinical trial at Ascension St. Ashwin Ravichandran and Scott Hittinger.
Pulmonary arterial hypertension, a form of high bloodpressure that occurs in the lungs, is a target of research by Cedars-Sinai investigators. We tried a fundamentally different approach--cell therapy delivered into the pulmonary artery--and found encouraging results, in patients already on combination conventional therapy."
Infusions of potentially therapeutic cells derived from the heart are safe for people with pulmonary arterial hypertension, a form of high bloodpressure that occurs in the blood vessels of the lungs and typically affects middle-aged women, according to a study led by Cedars-Sinai investigators.
High BloodPressure (Hypertension) Persistent high bloodpressure forces the heart to work harder to pump blood. Anemia Severe, untreated anemia can force the heart to pump more blood to compensate for the lower oxygen levels in the blood, potentially leading to enlargement.
Background Pulmonary embolism is a condition of right cardiac dysfunction due to pulmonary circulation obstruction. Malignant tumor-induced pulmonary embolism, which has a poor therapeutic outcome and a significant impact on hemodynamics, is the cause of sudden death in patients with malignant tumors.
In the 1980s, when Stella Kourembanas, MD, began her career in neonatology, she cared for newborns with pulmonary hypertension, a disease that results in abnormally high bloodpressure in the lung arteries and can lead to heart failure. But pulmonary hypertension still persists.
His bloodpressure was 180/110 mmHg and heart rate was 100 bpm. He had a high bloodpressure and heart rate and was initially treated with glyceryl trinitrate. If the dissection extends into the aortic arch branches, ensuring adequate cerebral perfusion during surgery is crucial to preventing stroke.
A drug approved to treat pulmonary arterial hypertension may be effective at managing hypertension and end-organ damage in patients with sickle cell disease, according to a new study. Preliminary efficacy data suggested the medication might improve heart function.
Introduction Multiple abnormal electrocardiographic findings have been documented in patients experiencing acute pulmonary embolism. To date, only a limited number of cases involving a complete atrioventricular block have been reported in acute pulmonary embolism. Echocardiography confirmed signs of right ventricular dysfunction.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the bloodpressure (lower afterload, which increases myocardial oxygen demand). The patient was put on a nitroglycerin drip and his pain improved with his bloodpressure.
He was in acute distress from pulmonary edema, with a BP of 180/110, pulse 110. He had diffuse crackles on exam and B-lines on chest ultrasound, and chest x-ray also confirmed pulmonary edema. Bloodpressure was 215/124 and HR 115 (on metoprolol). The hypertension alone is the likely etiology of the pulmonary edema.
On day 3 of hospitalization, he experienced a syncopal episode and had acute worsening of hypoxemia that prompted a CT angiography of the chest which revealed bilateral, large clot burden pulmonary emboli with proximal thrombus in both the right and left main pulmonary arteries.
Background:Primary pulmonary arterial hypertension (PAH) is a disease affecting young subjects. hypoxic animals developed PAH with peak RV systolic pressures (RVSP) being significantly higher than normoxic WT and hypoxic WT and hypoxic KO mice. Circulation, Volume 150, Issue Suppl_1 , Page A4117657-A4117657, November 12, 2024.
Finerenone, chronic obstructive pulmonary disease, and heart failure with mildly reduced or preserved ejection fraction: An analysis of FINEARTS-HF during the session "Finerenone: A Promising Addition to the Armamentarium or Merely an Academic Exercise?"
SCAPE is an acronym for sympathetic crash acute pulmonary edema, which can typcially occur in Pickering syndrome with renal artery stenosis [1]. Another term for transient acute pulmonary edema which occurs in renal artery stenosis is flash pulmonary edema. Sympathetic crashing acute pulmonary edem a. Prog Cardiovasc Dis.
Risk factors for PAD include smoking; having Type 1 or Type 2 diabetes, high bloodpressure, high cholesterol, chronic kidney disease, atherosclerosis in other parts of the body (such as coronary artery disease); and being age 75 years or older. and Global Data From the American Heart Association.
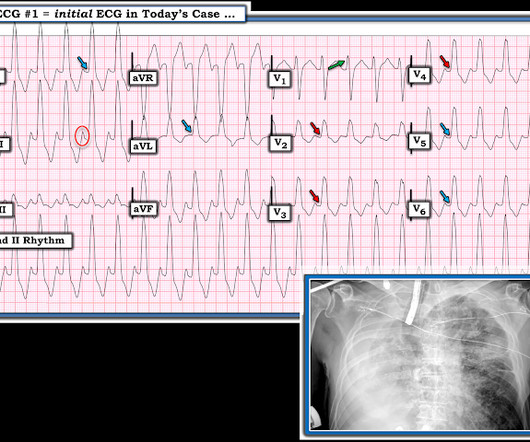
MY Thoughts on this CASE: Not being there — I am unaware of physical exam parameters ( bloodpressure, respiratory rate; oxygen saturation; heart and lung auscultation, etc. ). For a 10-minute video review on reading Pulmonary CT Scan — WATCH_this_VIDEO by Dr. Jake Gibbons. Figure-1: The initial ECG in today's case. (
This may be in the strength of the pulse ( or the bloodpressure recorded ) — or it may be in one or more waveforms in the ECG recording. The term "alternans" itself — merely indicates that there is a phasic fluctuation in some cardiac signal fro m one beat to the next within the cardiac cycle.
Given patient's acute drop in his bloodpressure, the patient was cardioverted with synchronized cardioversion at 200 J with no change in his rhythm. Here is a normal LBBB: In LBBB, monophasic wide R-waves should be limited to the lateral leads in left bundle branch block, as in this ECG.
At 37 weeks of pregnancy, I began having high bloodpressure and my doctor decided it was time to bring Austin into the world early. However, at the time, we did not know he also had a very rare isolated left pulmonary artery (causing PPHN) as this was hard to detect on the ultrasound and would later be detected at his cath.
EIH was defined as systolic bloodpressure (BP) at peak exercise >210 mm Hg in men or >190 mm Hg in women.RESULTS:In this prospective cohort study, we assessed patients with COA (n=41, age 4314 years, 26 [63%] men) and healthy controls (n=41).
Invasive arterial and pulmonary arterial measurements were obtained the first 72 hours after admission, and perfusion pressure, cardiac index and cardiac power output were calculated. Patients were classified according to SCAI class upon hospital admission.
Longitudinal bloodpressure was evaluated by tail cuff.Results:Compared with Ctrl, HFD/L-NAME mice showed cardiac remodeling, preserved systolic function and moderate diastolic dysfunction characterized by inverted or pseudonormal profiles and higher filling pressure (E/A=1.2±0.04 vs. Ctrl), indicative of pulmonary congestion.
We considered attempting electrical cardioversion to improve bloodpressure, but I suspected that he is in chronic atrial fibrillation that would be resistant to cardioversion, either electrical or chemical. The estimated pulmonary artery systolic pressure is 23 mmHg + RA pressure. l/min cardiac output.
Endotronix took a big step toward its vision for pulmonary artery pressure-based heart failure medication optimization, releasing positive results from its Cordella Sensor’s PROACTIVE-HF pivotal trial. mmHg decrease in seated mean PA pressure 5.9 mmHg decrease in-office systolic bloodpressure 2.2
Larger ASDs, on the other hand, may increase the risk of complications, such as stroke, arrhythmias or irregular heartbeats, pulmonary hypertension, or high bloodpressure in the lung arteries. Complications Of ASD The good news is small ASDs aren’t usually a cause for concern and close during infancy.
Aprocitentan (Tryvio) Approved: March 20, 2024 Indication: Hypertension in adults Administration: Oral Mechanism: Endothelin A and B receptor antagonist Developer: Idorsia Pharmaceuticals Significance: First and only FDA-approved endothelin receptor antagonist for high bloodpressure that remains uncontrolled with existing treatments.
How should we dose nitroglycerin to maximize its effects without dumping the bloodpressure in patients with SCAPE and those without SCAPE? How should we interpret the C3PO trial in the context of the world's literature on NIPPV in acute heart failure?
Finerenone, chronic obstructive pulmonary disease, and heart failure with mildly reduced or preserved ejection fraction: An analysis of FINEARTS-HF during the session "Finerenone: A Promising Addition to the Armamentarium or Merely an Academic Exercise?"
Notice I did not say "pulmonary embolism," because any form of severe acute right heart strain may produce this ECG. This includes, but is not limited to, PE, asthma/COPD exacerbation, hypoxic vasoconstriction from pneumonia, acute pulmonary hypertension exacerbation. Differences of Pulmonary Embolism T-waves from Wellens' T-waves: 1.
The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) When you suspect pulmonary embolism due to large RV on POCUS, always look for right axis deviation and a large R-wave in V1 because the large RV may be entirely due to chronic RVH, not acute PE. 2) Norepinephine to support BloodPressure.
Given that there was such a high bloodpressure, it is possible that this is a type 2 MI (supply demand mismatch due to high oxygen demand when myocardium is pumping against such elevated bloodpressure.) No signs for aortic dissection or pulmonary embolus. --"Results were discussed with the ordering physician.
Low LV filling pressures are due to several etiologies, most commonly due to volume depletion (dehydration or hemorrhage), but also due to other etiologies including, but not limited to: mitral stenosis, pulmonary hypertension (chronic, or due to pulmonary embolism), or poor RV performance.
The initial bloodpressure was 80/palp with a heart rate of 104, respirations 20, oxygen saturations of 94% and a finger stick blood glucose of 268. In addition, the patient received 750 mL of fluid resuscitation with transient improvement of bloodpressure.
Bloodpressure was 180/80. There was no pulmonary edema or hypoxia. The patient was unconscious. He was intubated. He had a combined respiratory and metabolic acidosis, with pH 6.98, pCO2 of 65 and HCO3 of 15. K was normal. Cardiac Echo showed excellent hyperdynamic function. The computer read the QRS duration as 160 ms.
The bloodpressure was 110/60. The patient had been on a long drive, suggesting possible pulmonary embolism (this was unlikely given absence of tachyardia, hypoxia, or any other feature of PE), so we sent a d dimer. [We Patients with ACS and acute pulmonary edema 3. It was not relieved by anything. This includes: 1.
On his physical examination, cardiac and pulmonary auscultation was completely normal. Bloodpressure: 130/80 mmHg, heart rate: 45/min, respiratory rate: 18/min, SaO2: %98, body temperature: normal. Bi-phasic scan showed no dissection or pulmonary embolism. He denies taking any medication.
Lungs are clear and there is no elevation in jugular venous pressure. Bloodpressure is within the goal as well. Clinical examination is consistent with a well-compensated patient. There are no signs of acute congestion.
Pericardial tamponade is also associated with pulsus paradoxus which is an abnormally large drop in systolic bloodpressure greater than 10 mmHg during inspiration. This may be in the strength of the pulse ( or the bloodpressure recorded ) — or it may be in one or more waveforms in the ECG recording.
Second , if the patient is hemodynamically stable, without pulmonary edema, it may be wise to try some fluids and and benzodiazepines and/or propofol for this post-seizure patient with likely high catecholamine levels. Place the Left Arm electrode on the 5th intercostal space, right sternal border. Monitor Lead I.
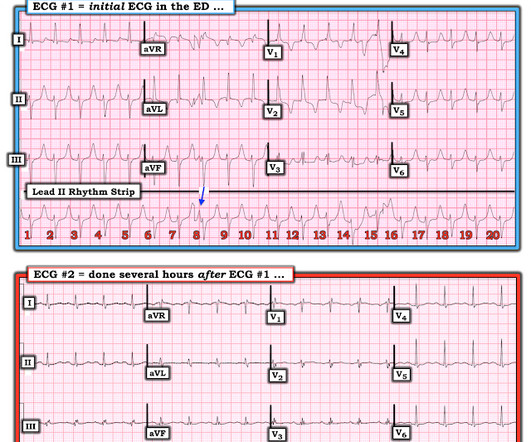
mEq/L A subsequent ECG was recorded several hours later, after the hemorrhage was controlled and the bloodpressure stabilized: Sinus rhythm with normal intervals, no RBBB, no LAFB, no long ST segment. The estimated pulmonary artery systolic pressure is 49 mmHg + RA pressure. mEq/L and 3.8
and angiotensin II type-1 receptor, SMC-MR contributes to myogenic tone and vasoconstriction, thereby contributing to systemic bloodpressure. By regulating expression of the L-type calcium channel subunit Cav1.2 While rarely tested, when sexes were compared, the mechanisms of SMC-MR-mediated disease were sexually dimorphic.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content