This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Current multi parameter monitors have invasive and non-invasive bloodpressure, respiration, pulse oximetry, pacemaker sensing and various other monitoring possibilities. Sometimes the number of alarms is so many that ICU staff may develop “alarm fatigue” and stop responding to alarms.
We report the outcomes of a 12-hour targeted-intensity monitoring (TIM) pathway for low-risk post-IVT patients.Methods:Post-IVT patients were considered low-risk if their NIHSS < 10, bloodpressure < 180/105 without medical intervention, level of consciousness was preserved, and no high-risk vessel stenosis/occlusion was present.
The 2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American Stroke Association states that we should control bloodpressure, reverse anticoagulation, and get the patient to a specialized inpatient stroke unit. 30 day readmission rate dropped to 3.23%Conclusions:Having
She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. She had an uneventful ICU course and was extubated for ongoing care with the inpatient psychiatric service.
Postoperatively, the patient was hypertensive to a systolic bloodpressure of 220 mmHg that was controlled with a nicardipine infusion that was gradually weaned off once the patient’s vitals were stable while in the Neuro‐ICU. CT‐guided biopsy of the L3‐L4 disc was also obtained.
The pacing rate was increased without clinical improvement and the patient was transferred to the ICU for closer monitoring/treatment. Therefore — Just because a patient remains awake and alert with an adequate bloodpressure for an extended period of time does not rule out the possibility sustained VT.
Despite heparin and supportive care, the patients mental status and bloodpressure worsened. She had an uneventful ICU course and improved steadily over the course of a week. NT pro BP returned at 10,676 pg/mL. She was diagnosed with massive PE and given intravenous tPA with rapid improvement in hemodynamics and mental status.
The cardiac monitor showed sinus rhythm but the automatic bloodpressure cuff was not reading. We arrived in the resuscitation bay and recorded a heart rate of 115 bpm and bloodpressure of 50/30 mm Hg. Why would she have such varying bloodpressure? She was discharged home in good condition.
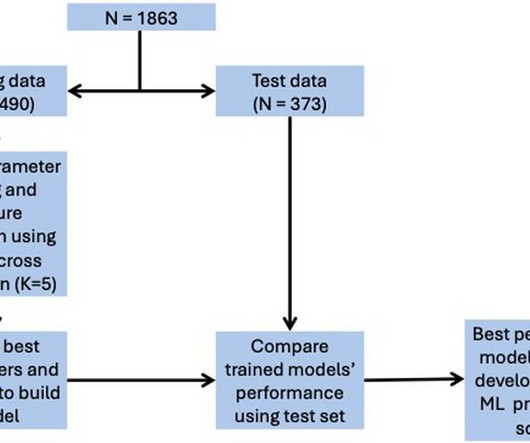
Final models were chosen to optimise area under the curve (AUC) score while ensuring interpretability.ResultsOverall, 128 (6.9%) patients died in hospital, with 292 (15.7%) patients requiring ICU admission and 373 (20.0%) patients with LVEF < 40%. for ICU admission, and 0.74 for in-hospital mortality, 0.78 for LVEF < 40%.
He was administered a therapeutic dose of low-molecular weight heparin and transferred to the ICU. Unfortunately, on day 8 of hospitalization, he became bradycardic with no recordable bloodpressures, and went into pulseless electrical activity soon after with an eventual demise.In
The arterial line bloodpressure immediately jumped from 80/40 with blunted monomorphic waveform to 140s/80s with bounding, normal-appearing waveform. He made it to the ICU, however the patient unfortunately expired approximately 24 hours after ICU admission.
Compartment pressures in the right calf were all 40-50 mmHg. At that time his diastolic bloodpressure was also hovering between 45 and 55 mmHg. Upon arrival in the ICU, before getting Continuous Veno-Venous Hemodialysis (CVVHD), his potassium had risen again to 7.8
On arrival in the ED, he was hypotensive with a systolic bloodpressure in the 70s. He was admitted to the ICU and transferred emergently to a facility where he could undergo emergent dialysis as a part of further evaluation and management. Fluid resuscitation was initiated. Here is the initial ED ECG: What do you think?
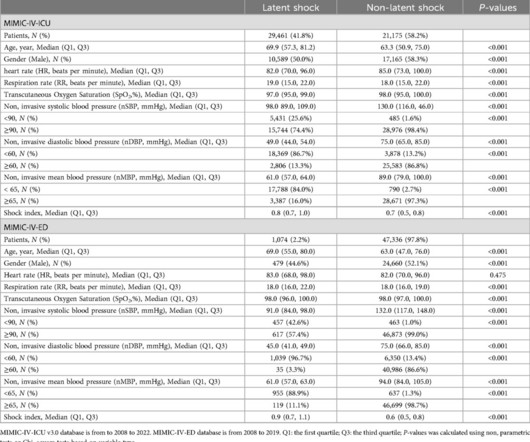
However, the usefulness of an ICU-based model to predict latent shock risk in an emergency department (ED) setting remains unclear. An adult noninvasive model was constructed based on the MIMIC-IV-ICU v3.0 Multiple regression analysis of the MIMIC-IV-ICU and MIMIC-IV-ED datasets showed mostly similar characteristics.
Orthostatic bloodpressures were recorded and confirmed orthostatic hypotension. The patient was transferred to the ICU on pressors, where a repeat bedside echo showed an LVEF of 10-15%. He suffered another cardiac arrest in the ICU with ROSC after another dose of epinephrine and one round of CPR.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content