This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BACKGROUND:It is unknown whether hypertensive microangiopathy or cerebral amyloid angiopathy (CAA) predisposes more to anticoagulant-associated intracerebral hemorrhage (AA-ICH). Among patients with AA-ICH, there were no differences in the proportion with lobar hemorrhage (63/148 [42.6%] versus 46/107 [43.0%]; OR, 1.02 [95% CI, 0.62–1.68];P=0.946)
Earlier SBP control was not associated with cardiac or renal adverse events.CONCLUSIONS:Our study confirms a clear time relation between early versus later SBP control (120–140 mm Hg) and outcomes in the one-third of patients with intracerebral hemorrhage who attained sustained SBP levels within this range.
Background and Purpose:2022 Intracerebral Hemorrhage (ICH) guidelines encourage treatment of bloodpressure (BP) as soon as possible following identification of ICH. Stroke, Volume 56, Issue Suppl_1 , Page AWP102-AWP102, February 1, 2025.
Background:The deleterious effects of intensive bloodpressure (BP) lowering in patients who achieved successful reperfusion may result from high BP variability (BPV). Stroke, Volume 56, Issue Suppl_1 , Page A119-A119, February 1, 2025.
Introduction:The 2022 AHA/ASA Guidelines for Intracerebral Hemorrhage (ICH) recommend initiating treatment and lowering bloodpressure (BP) within 2 hours of ICH onset and reaching the target systolic BP of 130-150mmHg within one hour of treatment initiation. Stroke, Volume 55, Issue Suppl_1 , Page ANS3-ANS3, February 1, 2024.
Background:Systolic bloodpressure (SBP) fluctuation is linked to increased death or disability in intracerebral hemorrhage (ICH) patients. Stroke, Volume 56, Issue Suppl_1 , Page A85-A85, February 1, 2025.
Introduction:Prospective studies and secondary analyses from clinical trials have identified increased systolic bloodpressure variability (SBPV) as a risk factor for poor outcomes.
BACKGROUND:Data on systolic bloodpressure (SBP) trajectories in the first 24 hours after endovascular thrombectomy (EVT) in acute ischemic stroke are limited. 2.82]), intracranial hemorrhage (aOR, 1.84 [95% CI, 1.31–2.59]), Hypertension, Ahead of Print. 2.59]), mortality (aOR, 1.75 [95% CI, 1.21–2.53),
Background and Purpose:Intracerebral and subarachnoid hemorrhages comprise roughly 15% of all strokes but have a higher risk of mortality and morbidity than ischemic strokes. Controlling hypertension after a hemorrhage is the primary intervention to limit the risk of hematoma expansion (HE) and the sequelae of secondary injury.
Current guidelines for bloodpressure (BP) management in patients with intracerebral hemorrhage (ICH) recommend acute lowering of systolic BP (SBP) to 140 mm Hg with a maintenance goal of 130 - 150 mm Hg. Stroke, Volume 55, Issue Suppl_1 , Page AWP175-AWP175, February 1, 2024.
Background and Objectives:There are limited data evaluating the optimum bloodpressure (BP) goal post mechanical thrombectomy (MT) and its effect on outcomes of patients with large vessel occlusions (LVO). Methods:We searched the PubMed, and Embase to obtain articles related to bloodpressure control post MT through September, 2023.
Goal bloodpressure was defined as systolic bloodpressure <160. Median initial bloodpressure in the MSU was 190/99, which dropped to a median bloodpressure of 157/80 upon arrival to the hospital. The target bloodpressure goal was met much quicker in the MSU.
Introduction:The 2022 AHA/ASA Guidelines for Nontraumatic ICH recommend initiating bloodpressure (BP) reduction within 2 hours of onset and achieving a target systolic BP of 130-150 mmHg within one hour of initiating a BP medication. Stroke, Volume 56, Issue Suppl_1 , Page ATMP66-ATMP66, February 1, 2025.
Background:Optimal Bloodpressure management after thrombectomy for acute ischemic stroke and its association with clinical outcomes remains unclear. We performed this study to compare clinical outcomes between intensive systolic bloodpressure (SBP) control (<120-140mmHg) and conventional SBP control (< 180mmHg).Methods:In
The new analysis of the trial results, led by UVA Health’s Andrew Southerland , MD, found that high blood sugar shortly after thrombolysis – opening blocked arteries in the brain with a clot-busting drug – was associated with greater risk for potentially deadly brain bleeds, particularly in older patients with more severe strokes.
Intracerebral hemorrhage is the most serious type of stroke, leading to high rates of severe disability and mortality. Patients with intracerebral hemorrhage who fail to receive early aggressive care have worse outcomes, suggesting that an important treatment opportunity exists. Stroke, Ahead of Print.
Background and Issues:Timely identification and intervention are critical for positive outcomes in acute intracerebral hemorrhage (ICH) patients. Establishing clear time targets for getting imaging, initiating bloodpressure control, reversing anticoagulation, and admission to Neuro ICU led to a reduction in mortality and 30 day readmissions.
Background:Elevated bloodpressure (BP) is common after Intracerebral Hemorrhage (ICH) and is linked with increased morbidity and mortality, partly due to hematoma expansion. Stroke, Volume 56, Issue Suppl_1 , Page ATMP62-ATMP62, February 1, 2025.
BACKGROUNDAlthough postprocedure bloodpressure (BP) correlates with outcome in patients undergoing endovascular thrombectomy (EVT), the optimal target is unknown.METHODSWe performed a pilot randomized‐controlled clinical trial enrolling participants with persistently elevated BP after successful EVT.
Studies suggest increased hemorrhage risk in patients with BP ≥170 mmHg and greater BP variability.Methods:We performed a retrospective study with data from the Get with The Guidelines database and electronic medical record of all adult AIS patients treated with TNK at a Comprehensive Stroke Center from 6/2021 to 6/2023.
BackgroundA strong risk factor for intracerebral hemorrhage (ICH) is elevated arterial bloodpressure, which is known to vary by season, with highest values in winter months. Whether ICH can be prevented by better control of arterial bloodpressure in seasons with expected incidence peaks will require further studies.
BackgroundDelayed cerebral ischemia represents a significant contributor to death and disability following aneurysmal subarachnoid hemorrhage. In murine studies (n=30), the endovascular perforation model was predominantly used, while rat studies primarily employed intracisternal blood injection to mimic subarachnoid hemorrhage.
Therefore, ASPIRING (Antiplatelet Secondary Prevention International Randomized Study After Intracerebral Hemorrhage) aims to recruit 4148 ICH survivors to determine the effects of antiplatelet agents after ICH definitively overall and in subgroups. 0.87]) and might increase the risk of ICH (rate ratio, 1.67 [95% CI, 0.97–2.90]).
Background:Anticoagulation-associated intracerebral hemorrhage (AC-ICH) often results in death. Factors associated with DTT ≤ 60 minutes include white non-Hispanic race, higher bloodpressure, lower NIHSS, and a larger hospital size. Stroke, Volume 55, Issue Suppl_1 , Page A145-A145, February 1, 2024.
Introduction:Intracerebral hemorrhage (ICH) leads to the highest mortality among stroke patients. The checklist tracks bloodpressure (BP) management and calling a neurosurgery consult. Stroke, Volume 56, Issue Suppl_1 , Page AWP136-AWP136, February 1, 2025.
Background:The 2023 American Heart Association/American Stroke AssociationsGuideline for Management of Patients with Aneurysmal Subarachnoid Hemorrhage(SAH) support use of the Ottawa Rule to screen individuals at risk. Stroke, Volume 56, Issue Suppl_1 , Page ANS1-ANS1, February 1, 2025.
Introduction:Intracranial hemorrhage (ICH) is the most severe adverse effect of anticoagulation in atrial fibrillation (AF) patients. Stroke, Volume 56, Issue Suppl_1 , Page A49-A49, February 1, 2025. Hypertension, diabetes, hyperlipidemia, and chronic kidney disease are well-known cardiovascular risk factors for ICH.
Introduction:Intracerebral hemorrhage (ICH) incidence follows both seasonal and diurnal patterns noted in the literature. These differences have been attributed to variations in the coagulation cascade, bloodpressure, and sleep-wake cycle that all have their own noted rhythmicity. hospitals between 1/1/2020 and 12/31/2021.
Background:We have previously identified that hemoglobin decrements and new-onset anemia during an intracerebral hemorrhage (ICH) hospitalization is frequent, rapid, and associates with poor outcome. Stroke, Volume 55, Issue Suppl_1 , Page AWP176-AWP176, February 1, 2024. The mean age was 66.5 (SD were female. 0.99, p=0.04).
Introduction:Intracerebral hemorrhage (ICH) is associated with poor outcomes in part due to a lack of perceived sense of urgency. HE was defined as per revised criteria (33% relative or 6 mL absolute increase in ICH volume, or new presence or 1mL increase in intraventricular hemorrhage).Results:Among
Patients were admitted between 2013-2021 for ischemic and hemorrhagic stroke and had seen a PCP/PCAPP (primary care physician/primary care advance practice provider) in a regional health system or affiliated outpatient clinics using the EPIC electronic health record.
Outcomes of MSU management in patients with intracranial hemorrhage (ICH) have not been reported.Methods:We conducted a retrospective review of ICH patients enrolled in the Benefits of Stroke Treatment Using a Mobile Stroke Unit (BEST-MSU), a prospective multicenter controlled trial comparing MSU with standard EMS management (SM).
BACKGROUND:Cerebellar intracerebral hemorrhage (cICH) is often attributed to hypertension or cerebral amyloid angiopathy (CAA). to −7.30];P=0.001), and higher admission systolic bloodpressure (172 [146–200] versus 146 [124–158] mm Hg,P<0.001).CONCLUSIONS:Our Stroke, Volume 54, Issue 12 , Page 3074-3080, December 1, 2023.
Introduction:The rapid identification of acute intracerebral hemorrhage (ICH) in patients with symptoms of acute stroke is decisive for prehospital triage and initiation of targeted therapies. Glial fibrillary acidic protein (GFAP) is a highly promising blood biomarker indicating ICH.
Introduction:Oxidative stress plays an important role in both early brain injury and delayed cerebral ischemia after subarachnoid hemorrhage (SAH). There were no differences in bloodpressure or body weight between the two groups. Stroke, Volume 56, Issue Suppl_1 , Page AWP368-AWP368, February 1, 2025. P<0.05, Fig.
BACKGROUND:Smoking is a well-established risk factor for subarachnoid hemorrhage (SAH), and current smokers have an increased risk of SAH. Stroke, Volume 54, Issue 12 , Page 3012-3020, December 1, 2023. Smoking status (continuation or cessation) before the occurrence of SAH was evaluated using the repeated national health screening program.
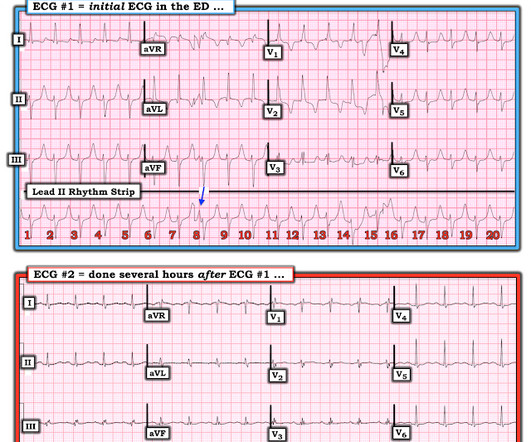
She had multiple rib fractures as well as serious hemorrhage and underwent massive transfusion. mEq/L A subsequent ECG was recorded several hours later, after the hemorrhage was controlled and the bloodpressure stabilized: Sinus rhythm with normal intervals, no RBBB, no LAFB, no long ST segment. mEq/L and 3.8
hours]); lower Glasgow Coma Scale scores (14 [IQR, 12–15] versus 15 [IQR, 14–15]); higher systolic bloodpressure 15 minutes before andexanet alfa bolus (mean, 151.6 hours [interquartile range (IQR), 1.2–4.3 hours] versus 3.7 hours [IQR, 1.6–7.0 mm Hg [SD, 24.1 mm Hg] versus 143.3 mm Hg [SD, 22.3 mL [IQR, 13.3–50.8 mL] versus 8.6
These clots can get dislodged and travel to blood vessels of the brain and block them, producing a stroke. Another reason for stroke is high bloodpressure. When the bloodpressure goes very high suddenly, small blood vessels in the brain may break leading to a bleed into the brain matter.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content