This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A projected rise in heart disease and stroke – along with several key risk factors, including high bloodpressure and obesity – is likely to triple related costs to $1.8 Smith Center for Outcomes Research in Cardiology and director of the cardiac criticalcare unit at Beth Israel Deaconess Medical Center in Boston, Mass.
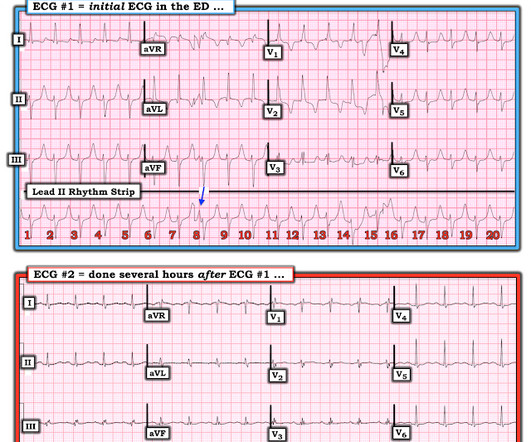
He presented to the Emergency Department with a bloodpressure of 111/66 and a pulse of 117. He was rushed by residents into our criticalcare room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. He had this ECG recorded.
He was brought to the criticalcare area where these rhythms were seen on the monitor: Wide complex tachycardia with no apparent P-waves, and very irregular Consistent with atrial fibrillation with aberrancy A Regular wide complex tachycardia. Still Irregular Bloodpressure during these rhythms was adequate; there was no shock.
Her initial troponin I, part of a criticalcare order set, returned at 0.55 mEq/L A subsequent ECG was recorded several hours later, after the hemorrhage was controlled and the bloodpressure stabilized: Sinus rhythm with normal intervals, no RBBB, no LAFB, no long ST segment. There were 2 K values measured in the ED: 3.7
The cardiac monitor showed sinus rhythm but the automatic bloodpressure cuff was not reading. While calling for some help and arranging to have her transported to our criticalcare zone, I got this quick ultrasound which confirmed my suspicion: This quick view was all I was able to obtain in the circumstances.
Bloodpressure is an important modifiable factor associated with poor neurological outcomes. Bloodpressure percentile was obtained based on age, sex, and the 50thheight range. We contrasted the bloodpressure with age and admission year matched CCCU controls without a history of stroke.
The patient arrived at the Emergency Dept criticalcare area and had this ECG recorded: The sinus bradycardia persists. Dr. Smith pointed out that while atropine may may result in slightly more oxygen demand, the increase in cardiac output and in bloodpressure would increase overall coronary perfusion and decrease ischemia.
On arrival in the ED, he was hypotensive with a systolic bloodpressure in the 70s. It is critically important for all EM and criticalcare providers to have an intimate understanding of hyperkalemia and its ECG findings. Fluid resuscitation was initiated. Here is the initial ED ECG: What do you think?
Ram Kumar The Society of Thoracic Surgeons Congenital Heart Surgery Database: 2021 Update on Outcomes and Research The Annals of Thoracic Surgery December 2021 Jennifer Nelson Capturing Adult Congenital Heart Disease: Framework for Development of an Adult Congenital Heart Disease Mortality Risk Model The Annals of Thoracic Surgery November 2021 Laura (..)
Ram Kumar The Society of Thoracic Surgeons Congenital Heart Surgery Database: 2021 Update on Outcomes and Research The Annals of Thoracic Surgery December 2021 Jennifer Nelson Capturing Adult Congenital Heart Disease: Framework for Development of an Adult Congenital Heart Disease Mortality Risk Model The Annals of Thoracic Surgery November 2021 Laura (..)
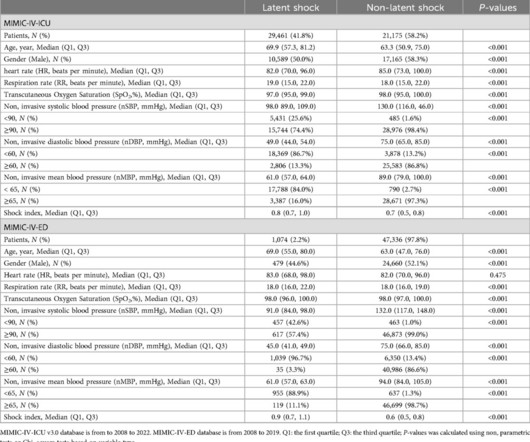
Its efficiency was compared with efficiency of testing with noninvasive systolic bloodpressure (nSBP) and shock index.ResultsA total of 50,636 patients from the MIMIC-IV-ICU database was used to develop the model, and a total of 2,142 patients from the Philips IntelliSpace CriticalCare and Anesthesia (ICCA)-ED and 425,087 patients from the MIMIC-IV-ED (..)
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the criticalcare area and the cath lab was activated. The bloodpressure was 170/100 in the criticalcare area.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content