This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
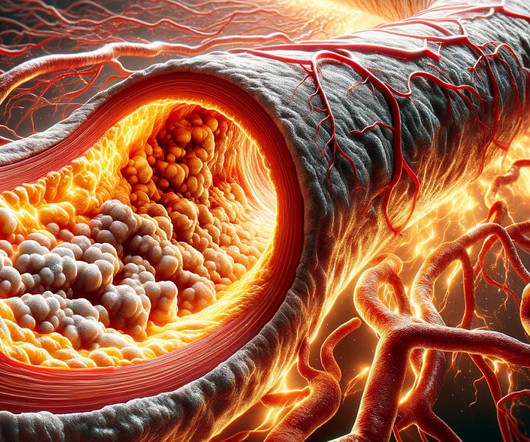
Reversing or regressing coronary artery disease is possible. You cannot eliminate the plaque entirely, but multiple clinical trials have shown plaque regression using high-intensity cholesterol-lowering treatments, which I have discussed previously. REVERSAL Investigators. 2004 Mar 3;291(9):1071-80.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the bloodpressure (lower afterload, which increases myocardial oxygen demand). The patient was put on a nitroglycerin drip and his pain improved with his bloodpressure.
Given that there was such a high bloodpressure, it is possible that this is a type 2 MI (supply demand mismatch due to high oxygen demand when myocardium is pumping against such elevated bloodpressure.) A CT Coronaryangiogram was ordered. LAD plaque with 0-25 percent stenosis.
The most accurate way (But not the only way) to answer this question is whether or not you have plaque in your coronary arteries. If you already have plaque, your risk of event an event goes up proportional to the amount of plaque you have 2. So, low risk by anyone’s books. in absolute risk terms.
Had bloodpressures a little on the high side. The key issue when it comes to the near-term risk of a heart attack is whether you already have coronary artery disease and how much of it. Subscribe now Cardiac CT There are two types of cardiac CT: CT Coronary Artery Calcium (CAC) Scan CT CoronaryAngiogram (CTCA).
A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. CT Coronary Artery Calcium Score Scan CT Coronary Artery Calcium Score CT CoronaryAngiogram As you can see from the above images, the CTCA provides far more anatomical detail.
Heart disease, the build-up of plaque in the coronary arteries, typically starts years, if not decades, prior to an event. The most common way to assess the presence and extent of coronary artery disease is with a CT scan, called a CT CAC score or CT CoronaryAngiogram. CT CoronaryAngiogram.
The bloodpressure was 170/100 in the critical care area. Cardiology wanted a CT of the aorta to rule out dissection, presumably partly due to the very high bloodpressure readings, but also because it is hard for people to believe that a 20-something woman could have acute thrombotic coronary artery.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content