This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
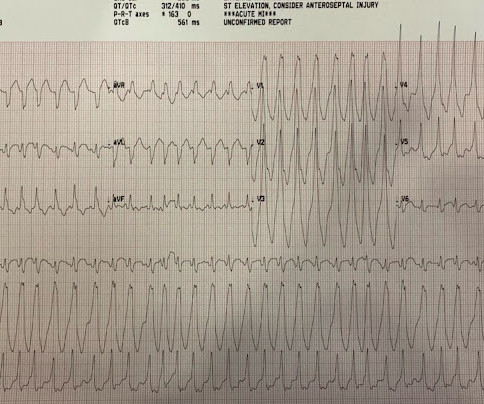
Mentation and bloodpressure were normal. He had no chestpain or shortness of breath. But it is not disorganized enough to be polymorphic ventricular tachycardia. Learning Points: Wide complex irregularly irregular tachycardias include PMVT, AF with WPW, and AF with aberrancy. What do you want to do?
Written by Bobby Nicholson MD and Pendell Meyers A man in his 30s presented to the ED for evaluation of chestpain and palpitations. The ECGs show a wide complex, irregularly irregular tachycardia. At this point, the patient had been symptomatic for almost 5 hours, appeared unwell with chestpain and diaphoresis.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. She presented to the emergency department after a couple of days of chest discomfort. Answer : The ECG above shows a regular wide complex tachycardia. Cardiac output (CO) was being maintained by the tachycardia.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. He is placed on heparin drip, he will have IV beta-blocker and oral beta blocker for heart rate control and bloodpressure management. He had received aspirin and nitroglycerin by EMS, with some improvement.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. The bloodpressure was 110/60. It was not relieved by anything.
This 54 year old patient with a history of kidney transplant with poor transplant function had been vomiting all day when at 10 PM he developed severe substernal crushing chestpain. He presented to the Emergency Department with a bloodpressure of 111/66 and a pulse of 117. He had this ECG recorded. Are the lungs clear?
They had already cardioverted at 120 J, then 200 J, which resulted in the following: Ventricular Tachycardia They then cardioverted at 200 J which r esulted in the same narrow complex rhythm shown above, at 185 beats per minute. This would treat both SVT or sinus tachycardia. I suggested esmolol if the heart rate did not improve.
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. 2) Norepinephine to support BloodPressure. An 80-something woman who presented with chestpain and dyspnea. Lots of info here.
Bloodpressure was 180/80. Here was his initial ECG: Regular Wide Complex Tachycardia. Differential of Wide Complex Tachycardia (check out this post) -- Sinus with aberrancy -- Aberrancy can be due to toxins (wide complex from the many drugs which have sodium channel blocking effects and prolong the QRS) --SVT with aberrancy.
MY Thoughts on this CASE: Not being there — I am unaware of physical exam parameters ( bloodpressure, respiratory rate; oxygen saturation; heart and lung auscultation, etc. ). I see the following: There is sinus tachycardia ( upright P wave with fixed PR interval in lead II ) — at the rapid rate of ~130/minute.
Dr Sanjay Gupta, a consultant cardiologist at York Hospital, is an expert in POTS, or postural tachycardia syndrome. The condition can leave sufferers debilitated, constantly exhausted, and sometimes unable even to walk. And like Long Covid, POTS often develops following a viral or other infection, Dr Gupta says.
His previous echo one month prior shows the same thing: “consistent with old infarct in LAD vascular territory, with EF 45%” "I think there is something else causing his tachycardia which is exaggerating his EKG findings and mimicking an acute myocardial infarction." The patient spontaneously converted back to sinus tachycardia.
He had no chestpain. The computer read is: **Acute MI ** The protocol for prehospital activation in the EMS system that this patient presented to requires 2 elements: 1) Chestpain 2) A computer read of **Acute MI ** Only 1 of 2 was present, so there was no prehospital activation. The patient was transported to the ED.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
The findings include sinus tachycardia, characteristic QRS morphology most diagnostic in V3 with a small R wave followed by a very large S wave with a convex upward ST segment morphology, ST segment strain morphology in the inferior and anterior leads leading to deep symmetric T-wave inversion. What is the Diagnosis?
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia. MY Thoughts on the ECG in Figure-1: The rhythm in ECG #1 — is sinus tachycardia at ~125/minute.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The initial bloodpressure was 80/palp with a heart rate of 104, respirations 20, oxygen saturations of 94% and a finger stick blood glucose of 268.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think? PUSH THE LYTICS !
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. An Impella device was placed to maintain cardiac output and perfusion pressures.
Prior ECG on file: Sinus tachycardia, imperfect baseline, otherwise unremarkable. Triage ECG, with patient awake and complaining of right lower extremity pain: What do you see? Compartment pressures in the right calf were all 40-50 mmHg. At that time his diastolic bloodpressure was also hovering between 45 and 55 mmHg.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. On arrival in the ED, he was hypotensive with a systolic bloodpressure in the 70s. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain.
However, recent studies have observed that people below 40 are also experiencing heart attacks due to high bloodpressure, cholesterol, diabetes, smoking, obesity, a sedentary lifestyle, and social and mental stress. This indicates that restoring normal blood circulation as quickly as possible will result in less damage.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Vasovagal predisposition (warm crowded place, prolonged standing, fear, emotion, pain: (-1) 2.
Written by Hans Helseth A 34 year old man with no known medical history presented to the ED after an hour of chestpain. He described the pain as a mid sternal "burning sensation" and rated it 8.5 out of 10 at onset, but on presentation to the ED, reported that the pain had improved to 4.5. 10 chestpain.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Case 1: 20-something woman with chestpain Case 2: 50-something man with chestpain Case 1 A 20-something yo woman presented in the middle of the night with severe crushing chestpain. The bloodpressure was 170/100 in the critical care area. Which patient needs a CT Scan? Denies SOB.
He denied chestpain. A Chest X-ray did not show pulmonary edema. This ECG was recorded: It is difficult to appreciate P-waves, but I believe this is sinus tachycardia. It is correct that he did not have chestpain, but we must remember that fully 1/3 of full blown STEMI do not present with chestpain.
The ECG in Figure-1 was obtained from a middle-aged man who presents to the ED ( E mergency D epartment ) with 6 hours of chestpain. Figure-1: The initial ECG in today's case obtained from a middle-aged man with 6 hours of chestpain. ( He is hemodynamically stable. Figure-2: The first leads to catch my "eye".
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content