This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
High bloodpressure, also known as hypertension, is a common condition that affects millions of people worldwide. Understanding how high bloodpressure impacts your heart and learning to manage it can significantly reduce your risk of heart disease and improve your overall health. What Is High BloodPressure?
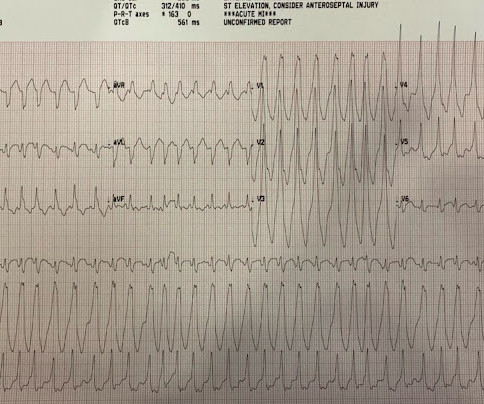
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. Here is the ED ECG (a photo of the paper printout) What do you think?
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Case An 82 year old man with a history of hypertension presented to the ED with chestpain at 1211. He described his chestpain as pleuritic and reported that it started the day prior while swinging a golf club. Another bloodpressure was checked. In lead I, about 1.5 mm of ST elevation has developed.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. He is placed on heparin drip, he will have IV beta-blocker and oral beta blocker for heart rate control and bloodpressure management. He had received aspirin and nitroglycerin by EMS, with some improvement.
A 50-something man presented in shock with severe chestpain. BP was 108 systolic (if a cuff pressure can be trusted) but appeared to be maintaining BP only by very high systemic vascular resistance. His prehospital ECG was diagnostic of inferior posterior OMI. The patient was in clinical shock with a lactate of 8.
A 50-year-old man presented to the emergency department with symptoms of acute chestpain, dizziness, and headache. His bloodpressure was 180/110 mmHg and heart rate was 100 bpm. He had a high bloodpressure and heart rate and was initially treated with glyceryl trinitrate.
Guidelines on hypertension (high bloodpressure) generally recommend measurement of bloodpressure in both arms in the initial visit. They also suggest that the arm with higher bloodpressure recording should be used to record bloodpressure in subsequent visits.
Mentation and bloodpressure were normal. He had no chestpain or shortness of breath. Written by Pendell Meyers A teenager was playing basketball when he suddenly developed palpitations and lightheadedness. He presented soon afterward at the Emergency Department with ongoing symptoms.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. The bloodpressure was 110/60. It was not relieved by anything.
After heart surgery, patients must focus on healing, gradually increasing activity levels, and monitoring vital signs, including bloodpressure. Pay attention to how your body responds, particularly monitoring for chestpain or unusual shortness of breath.
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. 2) Norepinephine to support BloodPressure. An 80-something woman who presented with chestpain and dyspnea. Lots of info here.
Written by Bobby Nicholson MD and Pendell Meyers A man in his 30s presented to the ED for evaluation of chestpain and palpitations. At this point, the patient had been symptomatic for almost 5 hours, appeared unwell with chestpain and diaphoresis. His bloodpressure was 118/96.
The patient reported no chestpain or shortness of breath. °C and a normal bloodpressure of 123/83 mm Hg. Clinical introduction A woman is her 60s with no medical history presented to the hospital with palpitations and occasional nausea. Observations revealed a normal temperature of 36.5°C
Here are some of the major ways in which chronic stress negatively impacts cardiovascular health: High BloodPressure When you experience stress, your body releases hormones like cortisol and adrenaline, which cause your heart rate and bloodpressure to spike.
High bloodpressure – Hypertension is a significant risk factor for heart disease. Routine bloodpressure checks are essential to maintaining a healthy heart as high bloodpressure often has no symptoms. Family history – If a close family member has had heart disease, it can raise your risk.
ET Murphy Ballroom 4 Comparison of an "Inclisiran First" Strategy with Usual Care in Patients With Atherosclerotic Cardiovascular Disease: Results From the VICTORION-INITIATE Randomized Trial Targeting Weight Loss to Personalize the Prevention of Type 2 Diabetes Once-weekly Semaglutide in Patients with Heart Failure With Preserved Ejection Fraction, (..)
There was no chestpain or SOB at the tim of the ECG: Computerized QTc is 464 ms A previous ECG from 8 years prior was normal. Absence of chestpain or SOB at the time of the ECG is important; had the patient had active chestpain, I would have recommended at least an emergency formal echo, if not cath lab activation.
Exercise helps strengthen your heart muscle, improves circulation, and lowers bloodpressure and cholesterol levels, all of which are crucial for maintaining optimal cardiac health. Smoking increases bloodpressure, reduces oxygen levels in the blood, and damages blood vessels, making it harder for your heart to function properly.
Manifestations of CVDs, such as chestpain, abnormal serum markers, unstable angina, myocardial infarction (MI), myocarditis, and new-onset hypertension, were documented. The most common symptom was left hemithorax and interscapular pain (317 patients, 46%).
He had no previous history of CAD, and presented with very typical waxing and waning chestpain, much worse with exertion but also present at rest and on presentation, though his pain was minimal at the time of the ECG. Bloodpressure was 150/80. I saw this 59 year old male 3 weeks ago.
Patient Mr. Paras Ram was having unstable angina (chestpain at rest) at his native place. Bhatnagar and his team did the entire surgery "anaortic", without touching the aorta (the great blood vessel of the heart), which is atheromatous at this age - thereby preventing the occurance of brain "stroke".
He had no chestpain. The computer read is: **Acute MI ** The protocol for prehospital activation in the EMS system that this patient presented to requires 2 elements: 1) Chestpain 2) A computer read of **Acute MI ** Only 1 of 2 was present, so there was no prehospital activation. The patient was transported to the ED.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
Be ready to give nitroprusside if the bloodpressure does go unacceptably high [ unopposed alpha in possible cocaine overdose is an overblown concern: see discussion below] Fourth , if it is AV nodal re-entrant tachycardia, sometimes a dose of 18 mg of adenosine is necessary. Marcus, G. Only beta-2 blockade (e.g., Hollander, J.
This 54 year old patient with a history of kidney transplant with poor transplant function had been vomiting all day when at 10 PM he developed severe substernal crushing chestpain. He presented to the Emergency Department with a bloodpressure of 111/66 and a pulse of 117. He had this ECG recorded.
MY Thoughts on this CASE: Not being there — I am unaware of physical exam parameters ( bloodpressure, respiratory rate; oxygen saturation; heart and lung auscultation, etc. ). Figure-1: The initial ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ).
In unadjusted analysis, factors significantly associated with troponin testing were a triage complaint of chestpain, older age, higher mean systolic BP, hypertension, diabetes, obesity, stroke or TIA, congestive heart failure, or coronary disease.
The gradual loss of elasticity in arterial walls and the presence of other risk factors, such as high bloodpressure and diabetes, contribute to the increased risk of cardiovascular disease (CVD) observed in aging populations. Risk factors such as smoking, chronic kidney disease, and aging can contribute to plaque formation.
Coronary arteries are blood vessels supplying oxygenated blood to the heart. As age advances and depending on risk factors like heredity, smoking, high bloodpressure and diabetes, fat build up occurs in these blood vessels. This can block smooth flow of blood and the person can develop chestpain.
Symptoms and Causes of Heart Murmurs The root cause of a heart murmur is abnormal or turbulent blood flow that occurs across your heart valves. It may be the result of anemia, an overactive thyroid, high bloodpressure, and other common conditions.
Additionally, coronavirus infection affects blood vessels, leading to inflammation, clotting, and potential compromise of blood flow to the heart. Yes, COVID-19 symptoms can resemble a heart attack, including chestpain, shortness of breath, and changes in echocardiogram or EKG. Can COVID-19 symptoms mimic a heart attack?
A middle aged man had off and on chestpain for 2 weeks, then 2 hours of more severe and constant pain. Just prior to transport, the patient became confused and agitated and, although bloodpressure and pulse were OK, I was worried about cardiogenic shock. He did not get prehospital activation. What do you think?
AFib causes a variety of symptoms, including fast or chaotic heartbeat, fatigue, shortness of breath, and chestpain, and causes about 450,000 hospitalizations each year, according to the Centers for Disease Control and Prevention.
Wellens' is a syndrome of a painless period following an anginal (chestpain) event. Chestpain, SOB, Precordial T-wave inversions, and positive troponin. She also complained of generalized weakness, lightheadedness, diaphoresis, chestpain, and cough. What is the Diagnosis?
The patient said his chestpain was 4/10, down from 8/10 on presentation. And, among our chief goals as medical providers — we want to treat pain when this can be safely done! Remember that patients with OMI can have normal ECGs! Repeat hsTnI was 183 ng/L, up from 26 ng/L. Around noon, cardiology was called for evaluation.
An unfilled heart is not able to pump out blood well and the bloodpressure falls. Inflammation of pericardium as inflammation elsewhere can be painful and cause chestpain. But pericardial effusion can build up slowly without much pain. This serious condition is known as cardiac tamponade.
These include breathlessness, chestpain, dizziness or even blackouts. Dysrhythmias are more likely in patients who are older and sicker with a larger burden of comorbidities such as diabetes, high bloodpressure, sleep apnoea and vascular disease. There are two other important points to note.
[link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left.
Bloodpressure was 180/80. Normal 0 false false false EN-US X-NONE X-NONE MicrosoftInternetExplorer4 Approach to Wide Complex Tachycardia Unstable – Shock it 12-lead if at all possible --Unstable defined by : ChestPain Shock Hypotension Very dyspneic Pulmonary Edema Stable Get a 12-lead ECG Sinus? He was intubated.
While fully acknowledging that "Sometimes ya gotta be there!" — in order to optimally assess the patient — the clinical definition of hemodynamic stability is for the patient to be without significant symptoms such as chestpain, shortness of breath, hypotension and/or mental status changes — as a direct result of the fast heart rate.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content