This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. The described rhythm was an irregular, wide complex rhythm.
Written by Pendell Meyers, with edits by Steve Smith Thanks to my attending Nic Thompson who superbly led this resuscitation We received a call that a middle aged male in cardiacarrest was 5 minutes out. No other cause of arrest was identified based on lab results or pan-CT scan.
One hour later (labs not yet returned), here is the ECG recorded just after the team noticed a sudden wide complex with precipitous decompensation, just before cardiacarrest: Bizarre, Brady, and Broad (wide QRS). Compartment pressures in the right calf were all 40-50 mmHg. Unfortunately, this was not recognized at this time.
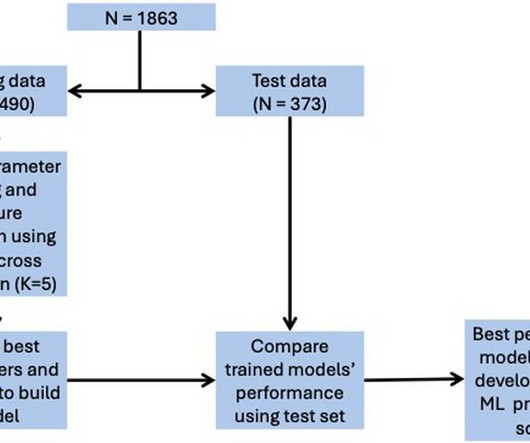
Final models were chosen to optimise area under the curve (AUC) score while ensuring interpretability.ResultsOverall, 128 (6.9%) patients died in hospital, with 292 (15.7%) patients requiring ICU admission and 373 (20.0%) patients with LVEF < 40%. for ICU admission, and 0.74 for in-hospital mortality, 0.78 for LVEF < 40%.
On arrival in the ED, he was hypotensive with a systolic bloodpressure in the 70s. He was admitted to the ICU and transferred emergently to a facility where he could undergo emergent dialysis as a part of further evaluation and management. Steve, what do you think of this ECG in this CardiacArrest Patient?"
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content