This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
People who experience out-of-hospitalcardiacarrest often require care at a regional center for continued treatment after resuscitation, but many do not initially present to the hospital where they will be admitted. Circulation, Ahead of Print. Many of these aspects can be delivered by protocol-driven care.
Background:Out-of-hospitalcardiacarrest (OHCA) is associated with unfavourable survival rates and neurological outcomes. Bloodpressure control is crucial in intensive care management, yet there are limited studies highlighting the influence of bloodpressure variability (BPV).
Out-of-hospitalcardiacarrest (OHCA) mostly occurs in crowded public places outside hospitals, such as public sports facilities, airports, railway stations, subway stations, and shopping malls. ECMO support therapy for patients with cardiacarrest can be considered when economic conditions permit.
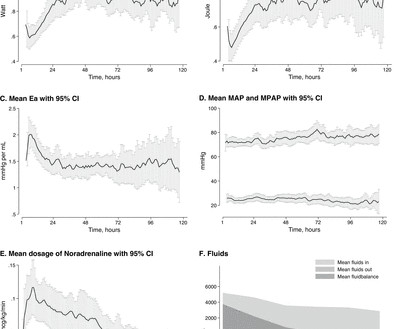
Background Circulatory failure after out-of-hospitalcardiacarrest (OHCA) as part of the postcardiac arrest syndrome (PCAS) is believed to be caused by an initial myocardial depression that later subsides into a superimposed vasodilatation. Results CPO, SW and oxygen delivery increased during the first 48 hours.
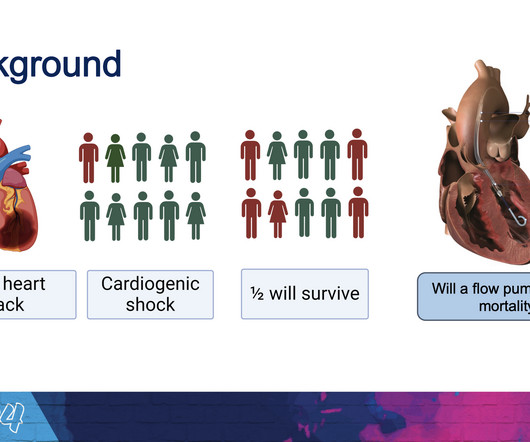
Cardiogenic shock after outofhospital cardiacarrest (OHCA) can be due to transient myocardial stunning but also reflect the increasing severity of ongoing heart failure. The Society for Cardiovascular Angiography and Interventions (SCAI) proposed a division of cardiogenic shock into 5 phenotypes, with cardiacarrest being a modifier.
I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiacarrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? Then the patient's electronic record from an outside hospital appeared. I wrote the following note in the chart: "V Fib arrest, has ICD.
Mechanical circulatory support (MCS) devices increase systemic bloodpressure and end organ perfusion while reducing cardiac filling pressures.Methods and ResultsThe National Cardiogenic Shock Initiative (NCT03677180) is a single‐arm, multicenter study. The primary end point was in‐hospital mortality. mm Hg, lactate to 2.7±2.8 mmol/L,
She was discharged after a short hospitalization with oncology and cardiology follow-up. Pericardial tamponade is also associated with pulsus paradoxus which is an abnormally large drop in systolic bloodpressure greater than 10 mmHg during inspiration. A repeat POCUS showed resolution of her pericardial effusion.
What is the utility of a head CT in cardiacarrest? We found intracranial hemorrhage in 2% of non-traumatic cardiacarrest patients, and in 4 others the presence of cerebral edema changed management. in Vienna found that 27 of 765 (4%) of out of hospitalcardiacarrests (OHCA) were due to SAH.
Written by Pendell Meyers We received a call from an outside hospital asking to transfer a "traumatic post arrest" patient. One hour later (labs not yet returned), here is the ECG recorded just after the team noticed a sudden wide complex with precipitous decompensation, just before cardiacarrest: Bizarre, Brady, and Broad (wide QRS).
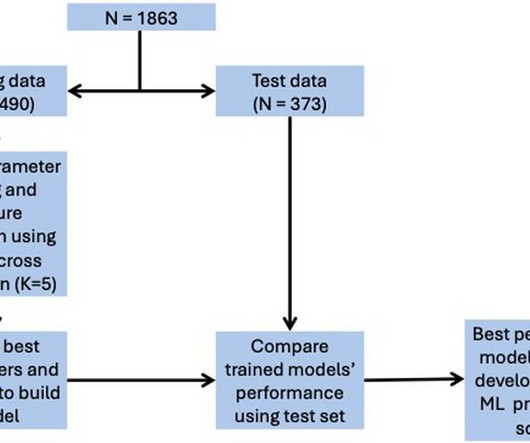
Final models were chosen to optimise area under the curve (AUC) score while ensuring interpretability.ResultsOverall, 128 (6.9%) patients died in hospital, with 292 (15.7%) patients requiring ICU admission and 373 (20.0%) patients with LVEF < 40%. for in-hospital mortality, 0.78 for ICU admission, and 0.74 for LVEF < 40%.
On arrival in the emergency department, invasive bloodpressure was 35/15mmHg and the patient was in profound cardiogenic shock with severe confusion secondary to brain hypoperfusion. The arterial blood gas showed a lactic acidosis with a lactate level of 17mmol/L. PUSH THE LYTICS ! The below ECG (ECG #4) was recorded.
In fact, most do not make it to the hospital alive, which explains why only a tiny percent of OMI are due to full LM occlusion. The Queen of Hearts gets it right here: Register for access to Queen of Hearts here The interventionalist stated that he could not do the procedure while the patient has a bloodpressure of 45 systolic.
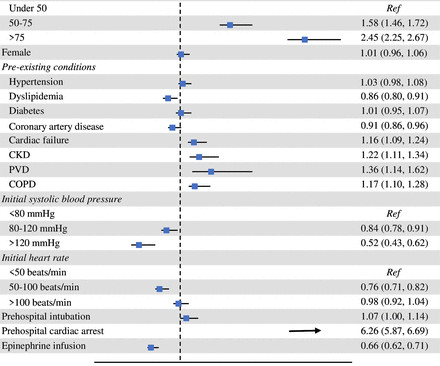
We aimed to describe the prehospital predictors of mortality in patients with non-traumatic shock transported to hospital by EMS. Reduced 30-day mortality was associated with administration of epinephrine (aHR=0.66, CI 0.62, 0.71) and systolic bloodpressures above 80 mm Hg in the prehospital setting.
Immediately after contrast injection into the LMCA, the patient had circulatory collapse, with a precipitous drop in bloodpressure. An Impella device was placed to maintain cardiac output and perfusion pressures. The patient was extubated on Day-3 of the hospital stay. Epinephrine infusion was begun.
Møller, MD , professor in the Department of Cardiology at the Odense University Hospital in Denmark, consultant at the cardiac intensive care unit of Copenhagen University Hospital Rigshospitalet and the study’s lead author. “I I think this will be a routine device that will be used in these desperately ill patients.”
alone, more than 800,000 of these people are at risk of MI and for approximately 200,000 of them, this may well be their second life-threatening cardiac event. Nearly 20% of those people who have had a MI will be hospitalized again within five years due to a second event.5 4 In the U.S. 12 Importantly, colchicine, 0.5
On arrival in the ED, he was hypotensive with a systolic bloodpressure in the 70s. A few days later an ECG was repeated which showed normal sinus rhythm with no further hyperkalemia findings: After a 3-week hospitalization for acute renal failure, hyperkalemia, and compartment syndrome, the patient was discharged to acute rehab.
AimThis study aimed to protect brain functions in patients who experienced in-hospitalcardiacarrest through the application of local cerebral hypothermia. Hemodynamic improvements included elevated systolic bloodpressure and heart rate, while left ventricular ejection fraction remained stable.
He had worked overnight the night before and presented to the hospital after his shift. His first recorded bloodpressure was 88/53 mm Hg. Forty five minutes later, his bloodpressure increased to 157/125 mm Hg, but his heart rate was now in the 30s. Here is his presenting ECG: What do you think?
Orthostatic bloodpressures were recorded and confirmed orthostatic hypotension. If the ventricular escape rhythm also gives out, the patient has cardiacarrest. He suffered another cardiacarrest in the ICU with ROSC after another dose of epinephrine and one round of CPR.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content