This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Former resident: "Just saw cath report, LAD stent was 100% acutely occluded." They of course opened and stented it. Acute MI per se usually does not depress cardiac function and bloodpressure enough to cause syncope ( Mostafa et al — J Com Hosp Intern Med Perspect 13(4):9-12, 2023 - ). Smith : "What was the outcome?"
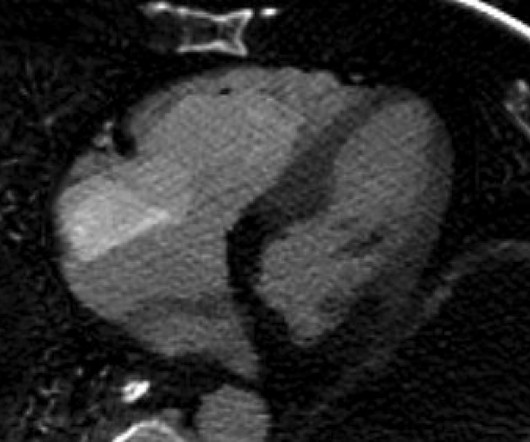
The ECG shows sinus bradycardia but is otherwise normal. On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions. OM before and after, arrow indicating stented region. The following ECG was obtained.
BP was 108 systolic (if a cuff pressure can be trusted) but appeared to be maintaining BP only by very high systemic vascular resistance. Here is his ED ECG: There is bradycardia with a junctional escape. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. What is the atrial activity?
Both of these features make inferior + RV MI by far the most likely ( Pseudoanteroseptal MI is another name for this ) There is also sinus bradycardia and t he patient is in shock with hypotension. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
Bloodpressure: 130/80 mmHg, heart rate: 45/min, respiratory rate: 18/min, SaO2: %98, body temperature: normal. His first electrocardiogram ( ECG) is given below: --Sinus bradycardia. The lesion was successfully stented. On his physical examination, cardiac and pulmonary auscultation was completely normal.
Patient 2 : 55 year old with 5 hours of chest pain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Smith : The fact that the ECG did not evolve is further proof that this was the baseline ECG. nearly identical to the first case).
They were unable to obtain a bloodpressure. His heart rate was in the low 20s and we were also unable to obtain a bloodpressure. He was given 50 mcg epinephrine with good response in both heart rate and bloodpressure. His rhythm on telemetry seemed to be sinus bradycardia vs junctional rhythm.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content