This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
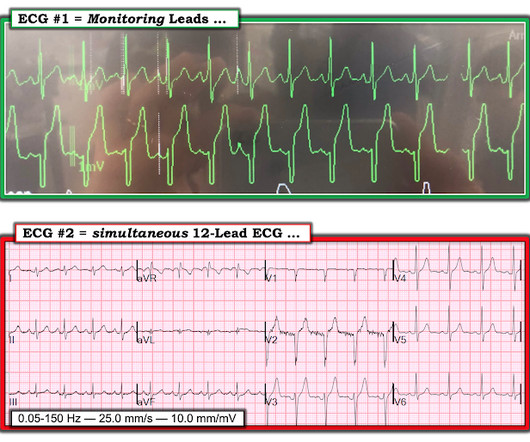
Resuscitation was initiated and this ECG was obtained: Likely AFib (irregularly irregular) with bradycardia. During this time, the patients bloodpressure continued to decline, requiring 4 pressors to sustain hemodynamics. In addition to marked bradycardia — could there be high-grade AV block?
He was hospitalized one week prior to EMS arrival for a seizure with no other recent illnesses or injuries. Bradycardia with “borderline hypotension” as described by the paramedics (BP 104/40) with 3-lead ECG as seen in Figure 1 were found. BVM was continued via NPA and the patient transported to the closest hospital.
That evening when he arrived home, he had an unexpected fall while getting out of the car, bloodpressure was reported to be 88/53. The patient and his wife suspected this was due to withholding of his midodrine and fludrocortisone during the hospitalization for his procedure. On the day of hospitalization, he had a CT scan.
Both of these features make inferior + RV MI by far the most likely ( Pseudoanteroseptal MI is another name for this ) There is also sinus bradycardia and t he patient is in shock with hypotension. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
On arrival in the emergency department, invasive bloodpressure was 35/15mmHg and the patient was in profound cardiogenic shock with severe confusion secondary to brain hypoperfusion. The arterial blood gas showed a lactic acidosis with a lactate level of 17mmol/L. PUSH THE LYTICS ! The below ECG (ECG #4) was recorded.
Immediately after contrast injection into the LMCA, the patient had circulatory collapse, with a precipitous drop in bloodpressure. An Impella device was placed to maintain cardiac output and perfusion pressures. The patient was extubated on Day-3 of the hospital stay. Epinephrine infusion was begun.
Written by Pendell Meyers We received a call from an outside hospital asking to transfer a "traumatic post arrest" patient. Compartment pressures in the right calf were all 40-50 mmHg. At that time his diastolic bloodpressure was also hovering between 45 and 55 mmHg.
On arrival in the ED, he was hypotensive with a systolic bloodpressure in the 70s. A few days later an ECG was repeated which showed normal sinus rhythm with no further hyperkalemia findings: After a 3-week hospitalization for acute renal failure, hyperkalemia, and compartment syndrome, the patient was discharged to acute rehab.
PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
He had worked overnight the night before and presented to the hospital after his shift. His first recorded bloodpressure was 88/53 mm Hg. Forty five minutes later, his bloodpressure increased to 157/125 mm Hg, but his heart rate was now in the 30s. Here is his presenting ECG: What do you think?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content