This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). This point is discussed in detail in the March 24, 2023 post of Dr. Smith’s ECG Blog ).
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI.
.: Cardiac cath was performed — and showed a distal LA D "culprit" lesion that was successfully stented. It may look identical t o the ST-T wave appearance seen after a STEMI with marked troponin elevation, that has now reperfused ( be this reperfusion spontaneous — or by treatment with PCI or thrombolytics ).
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
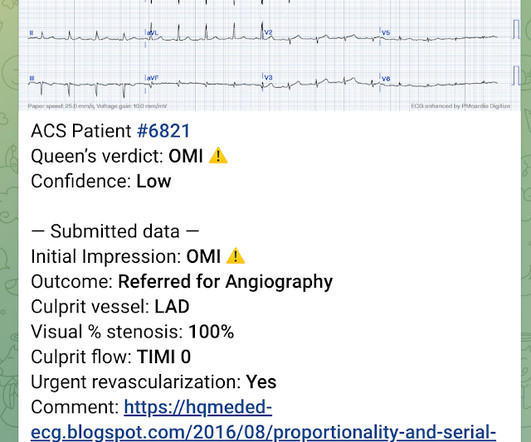
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
An undergraduate (not yet in medical school) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly arrived at work and happened to glance down and see this previously recorded ECG on a table in the ED. There was a 100% proximal LAD occlusion that was opened and stented.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion.
The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). I advised that perhaps posterior leads would help to persuade the interventionalist, since the 2022 ACC recommendations include posterior STEMI as a formal STEMI equivalent, but only officially by 0.5
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. Most large STEMI have peak troponin I in the 20.0 This was stented with a 2.25 Next trop in AM.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. It is stented with good angiographic result.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Successful drug-eluting stent placement opening up 95% mid RCA stenosis to 0% residual Nonobstructive left system disease. We have shown many examples of this on this blog.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Triage ECG: It was interpreted as lateral STEMI, and he was sent to the cath lab, where the angiogram showed unchanged CAD from known prior, with no acute culprit. His disease included 70% prox LAD, 80% distal LAD, 10% in-stent stenosis in the distal LCX, 70% OM1, 70% OM2, and 60% prox RCA. Described as a dull ache, 6/10 in severity.
This is all suggestive of posterior STEMI, but not definitely diagnostic. mm in only one posterior lead is highly sensitive and specific for posterior STEMI). Two stents were placed. ST depression in V1-V4, isolated, may be either posterior STEMI or NSTEMI. The ECG normalized overnight. Maximum troponin was 2.1
Subtle as a STEMI." (i.e., She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. This one is easy for the Queen.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. Cath lab was activated, and found a 95% proximal LAD occlusion which was stented. It’s unclear if the paramedic ECGs were seen or missed in the ED.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. This was a presumed culprit and a stent was placed. Edited by Smith He also sent me this great case.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
The lesion was successfully stented. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. If this patient was managed according to the STEMI/NSTEMI paradigm (although he would be a candidate for early invasive treatment), he would probably be taken to the cath lab hours later. Turk Kardiyol Dern Ars.
Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." He diagnosed anterior "STEMI" and activated the cath lab. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria. Two stents were placed with resultant TIMI 3 flow. What do you think? Of course not.
Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." They found 100% acute mid-LAD Occlusion MI, stented with excellent angiographic result. Learning Points: STEMI criteria misses 25-40% of OMI, like this case for example. mm of the "required" 1.0
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. It was stented. This was a large OMI.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. An open 90% LAD was stented.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Here is the angiogram after stent placement. Immediate versus delayed invasive intervention for non-stemi patients. Marinkovic, J.,
This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria. You can find the variables used to calculate the value on MD calc here: [link] Utilizing Dr. Smith’s Subtle Anterior STEMI Calculator (4-Variable), the value is greater than 18.2 The culprit mid LAD lesion was stented.
She was treated for NonSTEMI with antiplatelet and antithrombotic agents and went to cath the next day, where an where multiple LAD thrombi were found and the lesion will be stented. Waiting to cath a transient STEMI can be hazardous. See this case in which I made that mistake. Learning Points: 1.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? This was stented. Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below).
I would expect that a stent would be placed. The angiogram showed an open artery with 95% stenosis and thrombosis and it was stented. Quiz : What percent of full blown STEMI have an open artery with normal flow at angiogram? It too is "normal" and you decide that this is not OMI or STEMI and you just decide to get troponins.
At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). RAO Caudal View Post PCI This is the RAO Caudal view after thrombectomy and stent placement. Regular readers of this ECG Blog will be well familiar with many of these points. RAO Caudal view: This is the RAO Caudal view.
Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. It must have re-occluded between the ED and the cath lab) --Lesion was stented. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.)
Validation of the Modified Sgarbossa Rule for Diagnosis of STEMI in the Presence of Left Bundle Branch Block. There is no ST depression in lead I, which suggests a circumflex lesion The cath lab was activated and a circumflex occlusion was opened and stented, with a door to balloon time of 3 hours. Limkakeng AT. Theiling BJ.
The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented. The Non-STEMI, which was an OMI, was diagnosed much faster with AI on the ECG than with troponin. For more on ECG findings in pulmonary disease — Check out My Comment in the May 31, 2024 post in Dr. Smith's ECG Blog ).
Evidence regarding intervention to non-culprit plaques is mixed and beyond the scope of this blog post. On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions. Heitner et al. DOI:10.1161/CIRCINTERVENTIONS.118.007305),
would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic." Can you diagnose an ACO (STEMI) when you also have LVH? The criteria of Armstrong et al. References 1.
Unfortunately, we do not have those images for review, but the operators described a ruptured LAD plaque and they stented this area, which ensures the stability of the plaque. The image on the left shows the LAD before intervention, and the red circled portion on the right indicates the stented region. A picture is worth 1,000 words.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. It was stented. These include: i ) appreciation of how problematic the definition of “acute STEMI” can be; and , ii ) illustration of how dependence on this definition may result in overlooking acute coronary occlusion.
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). He has a h/o of 3 vessel disease and stents and his pain has been on and off for days.
reports MI in 2001 with a stent placed in the "marginal" artery. First, this patient had a known stent in the "marginal" artery and thought he was having a heart attack. By definition, this is a non-STEMI because there is not 1 mm of ST elevation in 2 consecutive leads. Pain is similar, but associated with less SOB.
This is typical for subendocardial ischemia, not STEMI, and often means left main ischemia or 3 vessel ischemia. Right sided ECGs are best recorded in the context of inferior STEMI. Because of precordial ST depression, clinicians were also worried about posterior STEMI. A right sided ECG was recorded 3 minutes later.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. So there was 3-vessel disease, but with an acute posterior STEMI. There is no ST elevation. See the list below.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content