This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
By the P s, Q s, 3 R Approach ( which I review in ECG Blog #185 ): Lots of P waves are present — being well seen in the long lead II rhythm strip. This slight variation in sinus P wave regularity tends to be greater when a 2nd- or 3rd-degree AV block is present ( called ventriculophasic sinus arrhythmia — as shown in ECG Blog #344 ).
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). This point is discussed in detail in the March 24, 2023 post of Dr. Smith’s ECG Blog ).
Regarding ST-T Wave Changes in Figure-2: As per the title of today's ECG Blog — one KEY lead "tells the tale". R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #294 — Reviews how to tell IF the " culprit " artery has reperfused.
Voltage for LVH is satisfied — at least by Peguero Criteria ( Sum of deepest S in any chest lead + S in V4 ≥23 mm in a woman — as discussed in ECG Blog #73 ). In the October 15, 2022 post of Dr. Smith's ECG Blog — Drs. I've reviewed my approach to the ECG diagnosis of LVH ofte n ( See ECG Blog #245 — among many other posts ).
Easy LINKS — tinyurl.com/KG-ECG-Podcasts — [link] — Other ECG Audio PEARLS I previously made for my ECG Blog can be found in the right column of each page on this blog just below this icon — under, "ECG Audio PEARLS". I recently recorded a series of 4 podcasts regarding KEY concepts in ECG interpretation.
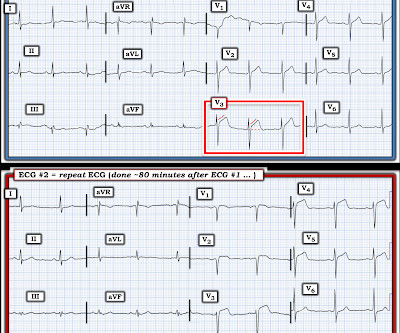
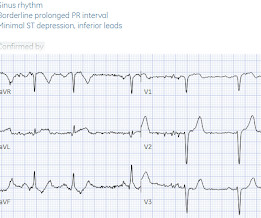
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
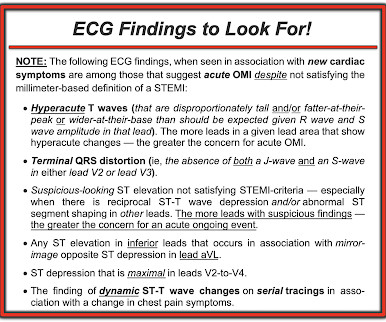
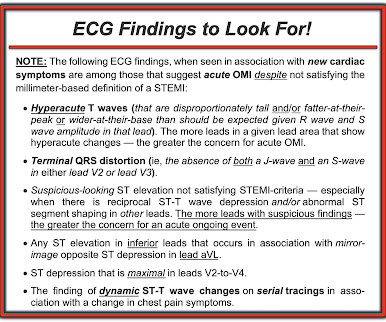
Doing so literally enables those of us who embrace the OMI Paradigm the ability to recognize within seconds that a patient with new CP ( C hest P ain ) — and — one or more hyperacute T waves — needs prompt cath regardless of potential absence of STEMI criteria. Figure-1: ECG from the August 26, 2009 post in Dr. Smith's ECG Blog.
As reviewed in ECG Blog #350 — t he clinical significance of Wellens' Syndrome — is that its recognition tells you that the patient has a high-grade LAD narrowing with presumably "hot" thrombus h avin g high propensity to propagate and/or totally occlude the LAD at any point in time ( including immediately ). What is W ellens’ S yndrome ?
PEARL # 1: Although seeing an elevated Troponin would provide additional support for immediate cardiac catheterization — the clinical reality is that the initial Troponin reading will not always be elevated in patients with acute coronary occlusion ( See March 24, 2023 post in Dr. Smith's ECG Blog ).
NOTE: As I've commented on in a number of previous blog posts — Wenckebach conduction may occur at more than a single level within the AV Node. R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #192 — The 3 Causes of AV Dissociation.
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. So the cath lab was activated. Long term outcome is unavailable.
MY Thoughts on the ECG in Figure-1: As always — I like to start my interpretation of 12-lead ECGs with assessment of the rhythm ( as per my systematic approach in ECG Blog-205 ). PEARL # 3: In the absence of an anterior STEMI — acute inferior MI is the result of either acute RCA or LCx ( L eft C ircumfle x ) coronary occlusion.
Based on ECG Blog #351 ( www.tinyurl.com/KG-Blog-351 ) LINK to this Page — www. tinyurl.com/KG-MedAll-351 — = = ECG Blog #205 = The Systematic Approach I favor. The "formula" = [link] LINK for Blog #205 = [link] - = Figure: The Systematic Approach that I favor. The talk will be recorded and posted on-line.
R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #193 — illustrates use of the M irror T est to facilitate recognition of acute Posterior MI. ECG Blog #294 — How to tell IF the "culprit" artery has reperfused.
Although this " Imbalance " of precordial T waves is not see n very often — in the “right” clinical setting, it has been associated with recent OMI ( O cclusion-based MI ) , most often from a LCx culprit artery ( See Manno et al: JACC 1:1213, 1983 — and the July 17, 2013 post by Salim Rezaie in ALiEM — and ECG Blog #350 ).
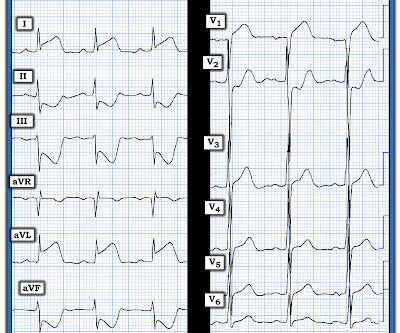
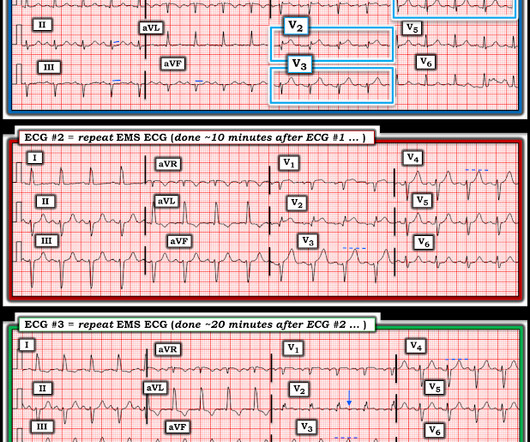
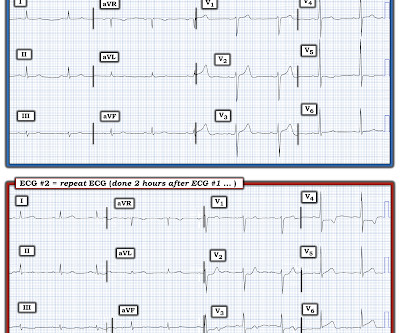
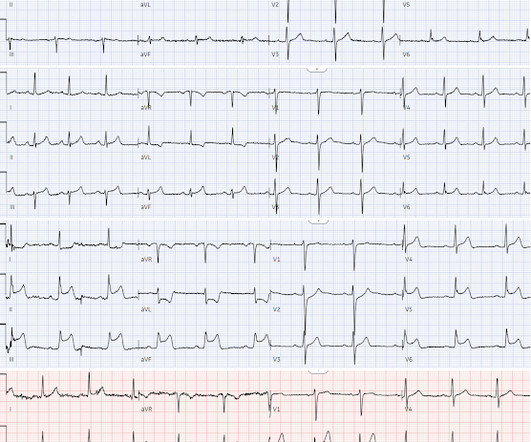
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
. = = R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #185 — Review of the P s, Q s, 3 R Approach for systematic rhythm interpretation. ECG Blog #271 — Reviews the concept of diffuse Subendocardial Ischemia. ECG Blog #316 — The patient died.
== P lease N OTE : After today — No new ECG Blog posts for 2- to -3 weeks. — I will also not be prompt in replying to emails. == All material on this ECG Blog site remains open! IF you scroll down a little on the right-hand column of this blog — You'll see a lot of icons. Figure-1: The initial ECG in today's case.
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
Although this " Imbalance " of precordial T waves is not seen very often — in the “right” clinical setting, it has been associated with recent OMI ( O cclusion-based MI ) from a LCx culprit artery ( See Manno et al: JACC 1:1213, 1983 — and the July 17, 2013 post by Salim Rezaie in ALiEM — and ECG Blog #350 ).
By the P s, Q s, 3 R Approach ( as reviewed in ECG Blog #185 ): The Q RS complex is obviously wide. R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #185 — Systematic P s, Q s, 3 R Approach to Rhythm Interpretation. I do not see P waves.
Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen. Meyers and Smith in the October 15, 2022 post of Dr. Smith's ECG Blog ). Restoration of sinus rhythm is evident in Figure-1.
In this ECG Cases blog we look at 9 patients with possible transient STEMI and discuss pitfalls and pearls in ECG interpretation and management. The post ECG Cases 39 – Transient STEMI Pitfalls and Pearls appeared first on Emergency Medicine Cases.
In this ECG Cases blog we present ECGs from 7 patients who presented with chest pain and mild anterior ST elevation. Can you identify which were early repolarization and which were anterior STEMI? The post ECG Cases 2: Early Repolarization or Anterior STEMI? appeared first on Emergency Medicine Cases.
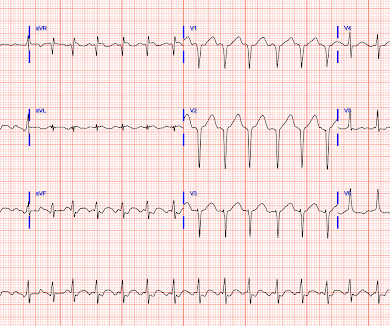
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. It is a mass delusion.
10 patients presented with the "STEMI-equivalent" ST elevation in aVR with diffuse ST depression. Jesse McLaren guides us through the differential diagnosis of ST elevation in aVR with diffuse ST depression in this ECG Cases blog. The post ECG cases 7: ST elevation in aVR, STEMI-equivalent? Which had acute coronary occlusion?
In this ECG Cases blog we look at 10 patients with shortness of breath, and discuss how the ECG can be used to help diagnose cardiac, respiratory and metabolic emergencies.
I came to work one day and one of my partners said, "Hey, Steve, we had a STEMI this afternoon!" That is not a STEMI. More cases can be found on the blog here. They had activated the cath lab and the interventionalist did not notice that it was not a STEMI/OMI. I said, "Cool, can I see the ECG?' He said: "What?
In this ECG Cases blog we look at 10 patients with potentially ischemic symptoms. Jesse McLaren explains 'Late STEMI' and how reperfusion strategies should not be based on time of symptom onset. The post ECG Cases 25: ‘Late STEMI’ – How acute is the coronary occlusion?
In this ECG Cases blog we look at seven patients with potentially ischemic symptoms and subtle ECG changes in the lateral leads. The post ECG Cases 4: Lateral STEMI or Occlusion MI? Which had acute coronary occlusion? Introducing the concept of Occlusion MI - a paradigm shift in ECG diagnosis of MI.
The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. For this reason, ECGs need first to be interpreted in isolation, and then applied to the patient. Could this false positive cath lab activation been prevented?
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
In this ECG Cases blog we look at 10 cases of patients with chest pain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach.
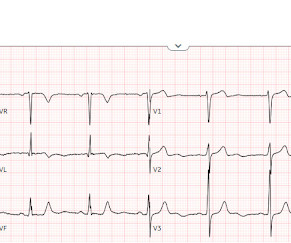
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? With serial ECGs that are ‘STEMI negative’ the physician could have waited for serial troponin levels or referred the patient as “non-STEMI”. What was the outcome and final diagnosis?
In this ECG Cases blog with Dr. Jesse McLaren we interpret 10 ECG cases and explore cardiac, metabolic and GI causes: We consider anginal equivalents, and look for ECG signs of Occlusion MI, including subacute occlusion from delayed presentations.
An undergraduate (not yet in medical school) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly arrived at work and happened to glance down and see this previously recorded ECG on a table in the ED. It was recorded at 0530: What do you think?
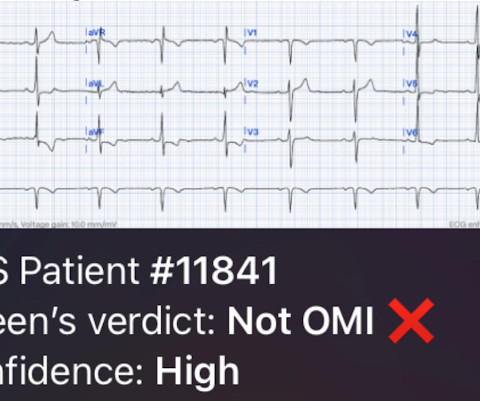
This is obviously unreliable data, as Dr. Smith’s Blog has published 51 cases of OMI with ECGs labeled ‘normal’ , 35 of which were identified by the Queen of Hearts – with 10 examples here. Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. What is the gold standard for ECG interpretation: patient outcome!!!
In this ECG Cases blog, Jesse McLaren and Rajiv Thavanathan explore how ECG and POCUS complement each other for patients presenting to the emergency department with shortness of breath or chest pain. They explain complementary diagnostic insights into pericardial effusion and cardiac tamponade, occlusion MI and RV strain.
Although there are more criteria to consider when looking for OMIs compared to STEMIs, anyone can learn them, and this guide is intended to help accelerate that process! Mark Hellerman — for his excellent work in producing the OMI Pocket Guide , that is the subject of today’s post on Dr. Smith’s ECG Blog.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content