This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion). The rhythm in ECG #1 is regular and supraventricular at a rate of ~75/minute. What is T-QRS-D?
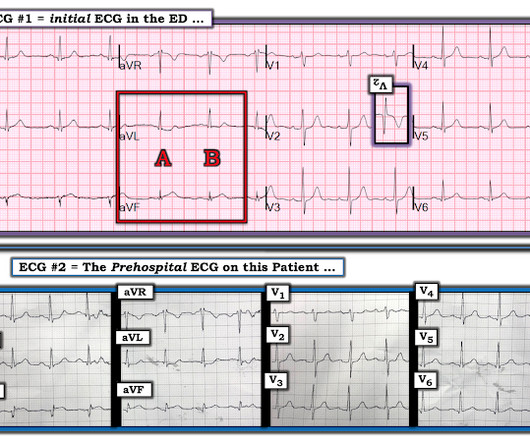
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. Thus, intracoronary imaging modalities are crucial in this setting. From Gue at al.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved.
This is as clear a STEMI as you can get. So this is classic inferoposterior STEMI on the ECG but is NOT acute coronary syndrome! The ECG and ultrasound could not have been differentiated from acute plaque rupture with occlusion of the RCA. This is consistent with MI, though one cannot tell if it is new or old.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. It is not rare.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
It does, in fact, the STE meets STEMI criteria since there is 1 mm of in V4 and V5. This ECG was texted to me with no other information. I assumed the presentation was consistent with acute MI. What did I say? Activate the cath lab." The T-waves in V2-V6 are diagnostic. There is also some non-diagnostic STE in inferior leads.
Although it is statistically unlikely, multiple plaque ruptures are possible. On intravascular ultrasound (IVUS), the mid RCA plaque was described as "cratered, inflamed, and bulky," and the OM plaque was described as "bulky with evidence of inflammation and probably ulceration." Heitner et al. DOI:10.1161/CIRCINTERVENTIONS.118.007305),
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. As there was ruptured plaque, this is NOT Prinzmetal's angina. Here is his triage ECG: There is massive STE in V3-V6, and also STE in II, III, aVF.
To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! One of the most common is rupture of a non-obstructive plaque, with thrombus formation and OMI that spontaneously lyses and leaves a wide open artery. It can only be seen by IVUS.
This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. I believe the latter (type II STEMI) is most likely. Troponin I rose to 44.1 FFR can be useful.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
The treating physician contacted the cardiologist immediately, but the cardiologist was not convinced, mostly because of the minimal symptoms and partly because it is not the classic morphology of anterior STEMI due to persistently occluded LAD, which should have upright T waves. An initial troponin returned at 12 ng/ml.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion). Is there STEMI?
I am going to code this as an acute STEMI as he had transient ST elevation which started to evolve in the emergency department but I think this is most appropriately termed STEMI." When is it anterior STEMI? No formal echo was done, and EF was normal on ventriculogram during cath, with no obvious wall motion abnormalities.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Today, they viewed the angiogram and concluded that the thrombus at the mid RCA must have extended proximally from the culprit ruptured plaque, extending proximal to the RV marginal branch and temporarily occluding it.
Could this be Septal STEMI (STE in V1 and aVR, with reciprocal ST depression in V4-V6?), In Septal STEMI , transmural ischemia of the septum is recorded by the overlying lead V1 as ST Elevation. Lead III is also on the right and might manifest ST Elevation in Septal STEMI. with ADDED STE in III?
EMS recorded these ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. Patients with transient occlusion may manifest only transient STEMI on ECG.
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. 24 yo woman with chest pain: Is this STEMI? This is not "diffuse", this is simply anterior, lateral, and likely apical.
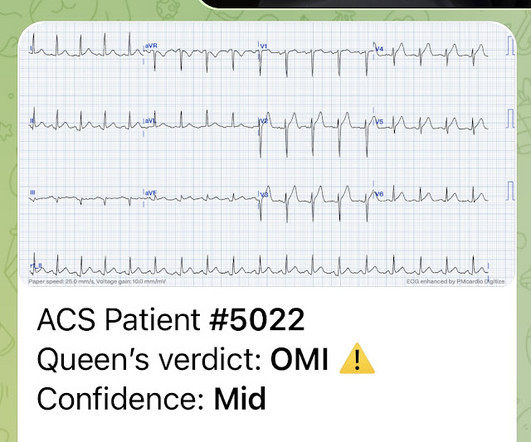
Prehospital Conventional algorithm interpretation: ANTERIOR INFARCT, STEMI Transformed ECG by PM Cardio: PM Cardio AI Bot interpretation: OMI with High Confidence What do you think? Mild Plaque no angiographically significant obstructive coronary artery disease. A 49 year old woman with h/o COPD only presented with sudden dyspnea.
Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. A recent study found that SCAD causes almost 20% of STEMI in young women. A study by Hassan et al. Lobo et al.
We have found in our study comparing inferior STEMI (manuscript in preparation) to inferior early repol several distinguishing characteristics. Nevertheless, even young people have atherosclerosis and plaque rupture. And young women have worse outcomes than other groups with STEMI because of the tendency to say, "Nah, couldn't be!"
LAD plaque with 0-25 percent stenosis. Later, she developed chest pain again, and had this ECG recorded: Obvious Anterior OMI that is also a STEMI Coronary angiogram- --Right dominant coronary artery system --The left main artery was normal in appearance and free of obstructive disease. --The A CT Coronary angiogram was ordered.
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. EKG is pictured below: What do you think?
This algorithm called it a STEMI. Yet it gave a diagnosis of STEMI. This is, in effect, a transient STEMI 2. It measured all the ST segments and recorded them (see bottom right) It only measure one lead (III) as greater than 1 mm, so there are not "2 leads with at least 1 mm". Learning points 1. They may be helpful.)
This is why it is essential that the OMI/NOMI paradigm replace the STEMI/NonSTEMI paradigm. Under Non-STEMI, this patient would not have intervention until at least 20 hours (next day), after the infarct is completed. Acute MI due to plaque rupture does happen in young people, including young women. Learning Points: 1.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). Therefore it means acute type 1 ACS plaque rupture with impeded flow and impending full occlusion until proven otherwise.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. Is that an obvious STEMI underneath that rhythm? Is this inferor STEMI? Atrial Flutter with Inferior STEMI? If I fix the rhythm will the ST changes resolve?
Of course, it is actually clearly an acute inferior MI, even though (as is so frequent) it does not meet "STEMI criteria." It was actually a dissection, not an atherosclerotic plaque rupture. I activated the cath lab and brought her to our stabilization room. I called the cardiologists to tell them that we have 2 acute MIs in the ED.
A "STEMI alert" was called and soon cancelled. This pattern occurs regardless of whether the cause is ACS (decreased supply) or any other cause of decreased supply or increased demand. There is a tiny hint of STE in aVL, but overall I do not think this looks like high lateral OMI. Pain lasted for approximately 45 minutes.
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. Patients with transient occlusion may manifest only transient STEMI on ECG.
It is equivalent to a transient STEMI. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL. Again, cath lab was not activated.
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow). He had multiple cardiac arrests with ROSC regained each time.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This was ruptured plaque with thrombus. She was a walk-in at triage.
Note: the 2022 ACC Expert consensus Chest pain guidelines state that "posterior STEMI-Equivalent" is a sign of acute coronary occlusion. 2/3 of STEMI have a peak 4th generation troponin I greater than 10.0 Comment: The first ECG is diagnostic of OMI that does not meet STEMI criteria. NSTEMI-OMI").
In my review of the literature, there are many articles which purport to demonstrate an acutely increased risk of plaque rupture from emotional stress, but I could not find any credible case reports that were not at least as likely to be takotsubo. Mechanisms of plaque formation and rupture. Coronary plaque disruption.
This was attributed to a "Type 2 MI", which is acute MI that is not due to ruptured plaque, but rather due to "supply demand oxygen mismatch". Most MINOCA is due to ruptured plaque with thrombus that lyses and does not leave behind a visible culprit. This is extremely elevated for a type 2 MI and totally consistent with STEMI.
The report describes heavy plaque in the proximal RCA by IVUS, but no lesions in the previously occluded RPL branch and no stent was deployed. Five days prior, she had a similar presentation to a different hospital. She underwent coronary angiography which showed thrombotic occlusion of an RPL branch s/p aspiration thrombectomy.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content