This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
As discussed in detail in ECG Blog #228 — this seemingly qualifies as a “ Silent ” MI ( Approximately half of those MIs not accompanied by CP — have some other associated symptom such as syncope, which substitutes as a “chest pain equivalent” ). Smith's ECG Blog ). ECG Blog #218 — Reviews HOW to define a T wave as being H yperacute ?
Stay tuned for our next blog, where we’ll outline actionable solutions to make prevention more effective and accessible. Enhancing Adherence: Simplify treatment plans and build trust through patient education. Driving Change in Clinical Practice: Support providers in adopting evidence-based interventions.
Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The pathologist may see a plaque that constitutes, for example, 50% of the cross-sectional area.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. It is not rare.
This blog explores how genetics influence heart health and whether mitigating these inherited risks is possible. Specific genetic variants, such as those affecting cholesterol metabolism, can increase the likelihood of plaque buildup in the arteries.
Although it is statistically unlikely, multiple plaque ruptures are possible. On intravascular ultrasound (IVUS), the mid RCA plaque was described as "cratered, inflamed, and bulky," and the OM plaque was described as "bulky with evidence of inflammation and probably ulceration." Heitner et al. DOI:10.1161/CIRCINTERVENTIONS.118.007305),
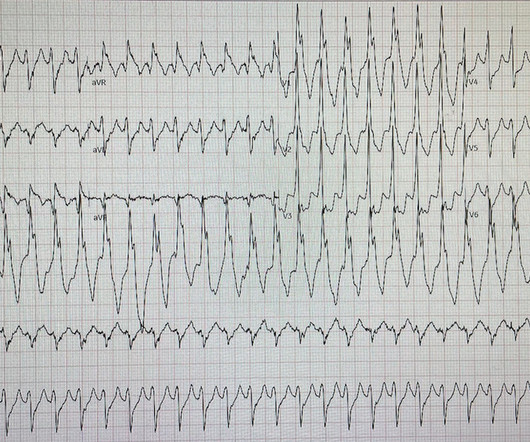
I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. Readers of the Smith ECG Blog will probably recognize this a very subtle inferior OMI. The VT vs SVT with Aberrancy debate is beyond the scope of this particular blog post.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. Thus, intracoronary imaging modalities are crucial in this setting. From Gue at al.
His ECG at the accepting facility is shown below: Accepting facility ECG The team reviewed his angiography films with an interventionalist and thought they were suspicious for plaque rupture in LAD, but they were not confident. The electrophysiologist is a reader of Dr. Smith's ECG Blog. They consulted EP for evaluation for ICD.
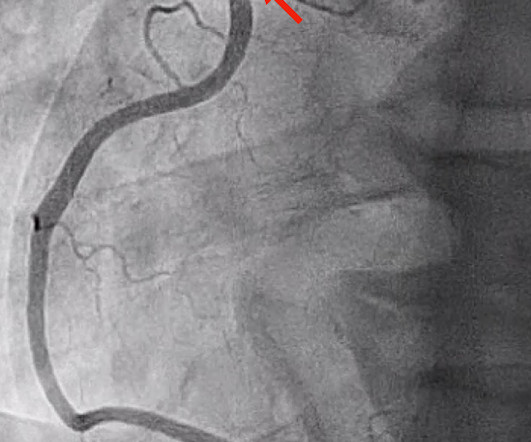
Angiography : --Culprit for the patient's unstable angina/Wellen syndrome is a ruptured plaque in the mid LAD. --As Despite description of Wellens’ Syndrome over 40 years ago — this syndrome remains misunderstood by all-to-many clinicians ( See My Comment at the bottom of the page in the August 12, 2022 post in Dr. Smith’s ECG Blog ).
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing? The ST depressions in I and aVL have resolved.
Smith comment : a very high proportion of MINOCA are ruptured plaque with lysed thrombus. That plaque is at risk of thrombosing again. It is worthwhile remembering that the majority of plaques which rupture are non-obstructive before they ulcerate and thrombose. Most plaque is outside the lumen!!
Learning Points: Type 1 MI is the type we are most familiar with: rupture of atherosclerotic plaque with production thrombus or platelet fibrin aggregates. You also appreciate the overly upright T waves in I and aVL which are reciprocal to the inferior T waves. But not all OMI is atherosclerotic in nature.
ECG 1 Readers of this blog will have no trouble recognizing this as an OMI with some early reperfusion. Possible etiologies (depending on your definition) include: plaque rupture with spontaneous recanalization, coronary artery vasospasm, spontaneous coronary artery dissection, or other rarer causes. < 0.033). His ECG is shown.
Because: 1) He has been reading this blog for a long time. The scan did not find PE, but showed evidence of coronary plaque: There are areas of dense white in the LAD (red and blue circles) and in the first diagonal (green circle). This is another case sent by the undergraduate (who is applying to med school) who works as an EKG tech.
And finally, after placement of a stent in the LAD: Before and after: (Unfortunately, this resulted in the "jailing" of the septal branches behind the stent and probably some degree of plaque shift which is why they do not opacify well in the "after" shot. This was the cost of preventing infarction of the anterior wall.) ng/mL (ref.
To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! One of the most common is rupture of a non-obstructive plaque, with thrombus formation and OMI that spontaneously lyses and leaves a wide open artery. It can only be seen by IVUS.
If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus." They often cannot even be recognized as culprits, as fissured or ulcerated plaque. FFR can be useful.
There are multiple possible clinical situations that could account for diffuse subendocardial ischemia that is not due to ACS and plaque rupture. The history in today's case with sudden loss of consciousness followed by chest pain is very suggestive of ACS and type I ischemia as the cause of the ECG changes.
Ramus: There is a large caliber branching ramus intermediate LAD is a medium caliber vessel that extends to the apex and is noted to have diffuse mild to moderate plaque in the midsegment. Post Procedure TIMI III. D1 is a medium caliber vessel, distal diagonal branches are small in caliber Echocardiogram Normal LV cavity size and thickness.
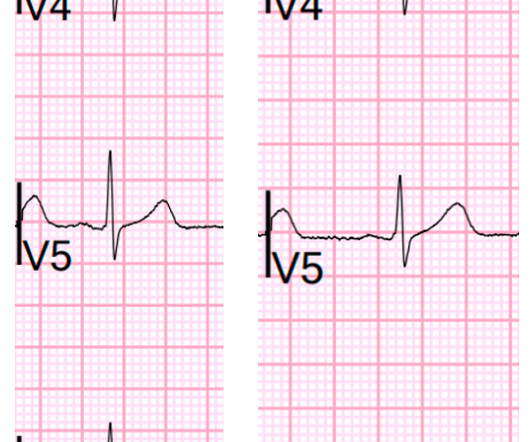
ECG 2 Especially in the context of the first ECG, readers of this blog will readily appreciate the ST elevations and hyperacute T waves in II, III, aVF, V6, and to a lesser extent V5. As an aside, the LCx OMI is a type 2 event, since it is due to supply-demand mismatch from thrombus, and not due to atherosclerotic plaque rupture or erosion).
In this blog, well explore why anemia can occur after heart bypass surgery, how common it is, and how it can be managed. This condition occurs when the blood vessels that supply blood to the heart become blocked or narrowed by plaque buildup. It can also be considered a postoperative complications may hinder recovery.
At AMS Cardiology we understand the significance of proactive care; that’s why we’ve put together this blog where we’ll explore the essential aspects of peripheral artery disease prevention and management. Medications – Medications play a crucial role in managing PAD symptoms.
With time, fat and cholesterol can get trapped in the areas of wear and tear and cause plaque formation. The plaques can damage us in 2 ways. Firstly the plaque may continue to build up and cause actually restrict blood from getting to the heart muscle and this often presents with symptoms of chest tightness on exertion or angina.
In this blog, we’ll break down the steps of coronary circulation, helping you understand how your heart maintains its own health while keeping the rest of the body alive and well. This is where coronary circulation comes into play. Any interruption in this process can result in serious consequences.
link] For those who have read my blog assiduously, or have read ‘The Clot Thickens’, none of this is new, or any surprise. The thrombogenic hypothesis, that endothelial damage and subsequent clot formation underlies the formation and growth of plaques, may represent a better model for ASCVD. Anyway, here it is. Here is the abstract.
Reperfusion of OMI indicates at least partial thrombolysis of occluding thrombus, but still unstable plaque rupture, which can reocclude at any moment. This case's first EMS ECG shows a rare example of LVH with active anterior and high lateral OMI. Comparison to prior ECG can be very helpful.
The diagnostic criteria of stress cardiomyopathy includes the presence of transient regional wall motion abnormalities (typically not in a single coronary distribution), absence of angiographic evidence of obstructive coronary disease/acute plaque rupture, with presence of new electrocardiographic abnormalities or modest troponin elevation.
Today, they viewed the angiogram and concluded that the thrombus at the mid RCA must have extended proximally from the culprit ruptured plaque, extending proximal to the RV marginal branch and temporarily occluding it. 24, 2018 ECG Blog — Please scroll down to the bottom of the page to My Comment, in the section "Beyond-the-Core". ).
There was a ruptured plaque with thrombus in the LAD, with some flow still (accounting for the inverted T waves). Another EKG was done at 0739: (#5) This shows even more ST elevation. The patient was still asymptomatic. An initial troponin returned at 12 ng/ml. The cath lab was activated.
Therefore it means acute type 1 ACS plaque rupture with impeded flow and impending full occlusion until proven otherwise. While subendocardial ischemia pattern can be due to any possible reason for supply/demand mistmatch in infinite clinical scenarios, this patient's scenario was acute chest pain consistent with ACS.
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. As there was ruptured plaque, this is NOT Prinzmetal's angina. It is just as dangerous, as there is a ruptured plaque with thrombus (which lysed) in the proximal LAD. Values: STE60V3 = 2.0, QRS V2 = 10, RAV4 = 15.5, There was good flow. It was stented.
Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. Angiography Angiography was performed after aspirin and heparin were started.
The ECG and ultrasound could not have been differentiated from acute plaque rupture with occlusion of the RCA. So this is classic inferoposterior STEMI on the ECG but is NOT acute coronary syndrome! This could not have been known without the angiogram.
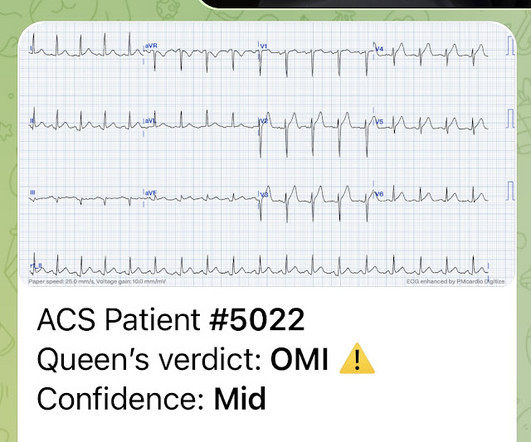
Mild Plaque no angiographically significant obstructive coronary artery disease. I looks as if there has been reperfusion. PM Cardio AI Bot: Not OMI with high confidence Angiogram: Speckle Tracking of Acute Pulm Edema.MOV from Stephen Smith on Vimeo.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
She had some very minor plaque but certainly nothing that could explain the heart attack and therefore she was discharged with a diagnosis of MINOCA i.e She agreed and we performed an angiogram and we were fully expecting a blockage but interestingly there weren’t any.
High cholesterol levels – Elevated levels of bad cholesterol can contribute to plaque buildup in your arteries, increasing the risk of heart disease. Routine blood pressure checks are essential to maintaining a healthy heart as high blood pressure often has no symptoms.
We’ve presented many variations on this theme on Dr. Smith’s Blog — with today’s case being distinguished by its discovery on abdominal exam ! For more on “My Take” for a systematic approach to ECG interpretation — Please check out My Comment at the bottom of the page in the October 17, 2022 post in Dr. Smith’s ECG Blog.
Only after her troponin peaked at 500,000 ng/L did she get her angiogram, which showed a 100% left main occlusion due to ruptured plaque. Young people can suffer acute coronary occlusion, whether by typical atherosclerotic plaque rupture, or by coronary anomalies, coronary aneurysms, dissections, spasm, etc. Diagnostic of Massive OMI.
Acute MI due to plaque rupture does happen in young people, including young women. Artificial intelligence (Convolutional Deep Neural Networks) will be able to discern this subtle information. Beware a low HEART score. It is only meaningful if you can accurately interpret the ECG. Here are 11 cases of young women with acute MI.
Dr. Punjabi has a fantastic radiology blog on Spectral CT: [link] A negative CT should not be relied upon to rule out ischemia. But young people do have MI, due to anomalous coronary arteries, coronary artery dissection, Kawasaki dz, even atherosclerotic plaque rupture, and other etiologies. Under 20, myocarditis is far more likely.
For example, a coronary plaque ruptures: the vessel can undergo occlusion, spontaneous reperfusion, maybe reocclusion, again reperfusion, etc. If this patient was discharged from the ED she very likely would have died. We must be the experts and pick up these life-saving ECG findings! ACS can be a very dynamic process.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content