This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The patient was discharged with a diagnosis of acute pericarditis — and treated with a full course of colchicine and ibuprofen. The ultimate discharge diagnosis was acute pericarditis. ( See ECG Blog #215 — for more on the Cabrera format. = From the information provided — I would not make the diagnosis of acute pericarditis.
Overall, this looks like one of the rare ECGs that is actually specific for pericarditis in my opinion. Pericarditis maybe." Meyers' words — "is one of the rare ECGs that is actually specific for pericarditis". ii ) Today's case emphasizes the importance of the history in making the diagnosis of pericarditis.
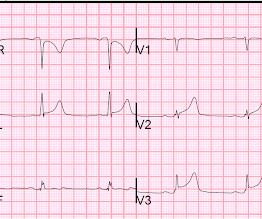
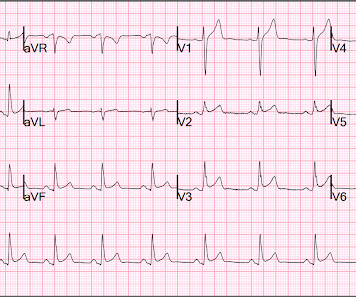
Pericarditis is rare — but myocarditis is not , so especially in this age group — more information is needed to quickly determine if this could be an acute MI, myocarditis, or none of the above. Does the patient's age infuence your interpretation? Figure-1: The initial ECG in today's case. (
Jesse McLaren guides us through 9 cases and explains how pericarditis is a diagnosis of exclusion through 3 simple steps: 1. Exclude complications of pericarditis, eg myocarditis, large pericardial effusion 3. Exclude normal variant ST elevation presenting with benign chest pain on this month's ECG Cases blog.
mm has been described in normal subjects) Overall impression: In my opinion and experience, this ECG most likely represents a normal baseline ECG, but with a small chance of pericarditis instead. I texted this to Dr. Smith without any information, and this was his reply: "This could be pericarditis but probably is normal variant."
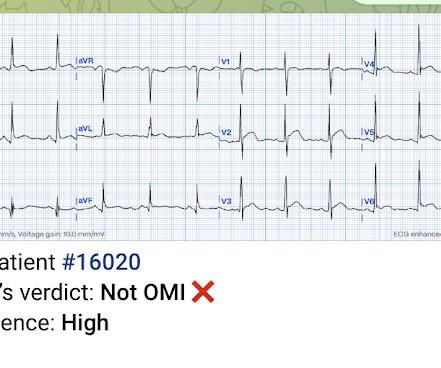
This ECG together with these symptoms is certainly concerning for OMI, but the ECG is not fully diagnostic, and another consideration could be acute pericarditis. Mistaking OMI for pericarditis is a much more harmful error than the converse. The rate is tachycardic, which is uncommon in OMI and common in pericarditis.
In this ECG Cases blog Dr. Jesse McLaren guides us through 10 cases, driving home the points that sepsis is a common cause of rapid Afib and diffuse ST depression with reciprocal ST elevation in aVR, myo/pericarditis is a diagnosis of exclusion, endocarditis or lyme carditis can cause AV block, PE can cause low grade fever and ECG signs of acute RV (..)
The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.” The final cardiology interpretation confirmed the computer interpretation of “ST elevation, consider early repolarization, pericarditis or injury”. A healthy 45-year-old female presented with chest pain, with normal vitals.
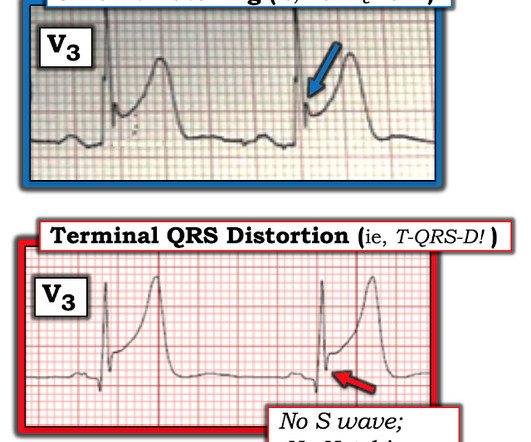
Clinician and EKG machine read of acute pericarditis. While it is true that inferior MI has ST depression in aVL 99% of the time (Bischof and Smith), and that inferolateral ST elevation is the most common distribution for pericarditis, the ST elevation in V3 has "terminal QRS distortion (TQRSD)," (diagnostic of LAD occlusion).
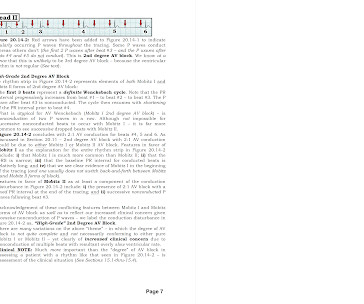
Assessing the Rhythm: I favor use of the P s , Q s , 3 R Approach for assessing the cardiac rhythm ( See ECG Blog #185 ). As emphasized in ECG Blog #326 ( and as I review in the ADDENDUM below ) — Mobitz I, 2nd-Degree AV Block ( ie, AV Wenckebach ) — is by far (!) ECG Blog #236 — Reviews the 3 Types of 2nd-Degree AV Block.
Here is his initial ED ECG: The R-wave in V4 extends to 33 mm, the computerized QTc is 372 ms The only available previous ECG is from one year ago, during the admission when he was diagnosed with pericarditis: 1 year ago ECG, with clinician and computer interpretatioin of pericarditis Normal 0 false false false EN-US X-NONE X-NONE What do you think?
But there was some doubt as to whether it might be pericarditis because of the ST elevation in I and II, without ST depression in III. Add that to "sharp" pain and a 33 year old, and it is easy to convince yourself that this is, indeed, pericarditis. This is a good sign for myocardial infarction and does not happen in pericarditis.
Pericarditis refers to inflammation of the pericardium The pericardium is a sac within which the heart sits. Acute inflammation of this sac is known as acute pericarditis. About 5% of patients who present to A+E with chest pain which is not deemed to be a heart attack or angina are ultimately diagnosed with pericarditis.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardial infarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). As already mentioned, this patient could have post-infarction regional pericarditis from a large completed MI. Sinus tachycardia has many potential causes. Hammill SC.
It is easy to say pericarditis in such a case. young male no risk factors and ST-elevation in several leads) As Dr. Smith has emphasized many times you diagnose pericarditis at your patient's and your own peril. Keep an eye on the blog as an OMI QUIZ soon will be published where you test yourself vs the Queen!
The undergraduate continues: This new EKG pattern is more suggestive of acute pericarditis. Usually with pericarditis, some degree of PR segment depression is expected. This is typical of pericarditis. But, as I always say, you diagnose pericarditis at your peril. This EKG seems to lack it.
There is a reasonable chance of pericarditis in this case, or this could be a baseline." Sadly, I did not receive enough information to adjudicate whether this patient has pericarditis or not. I sent this to Dr. Smith and this was his response: "Likely pericarditis, but that is perilous. I immediately responded: "cool fake!
Pericarditis? If you were thinking that this is pericarditis, that would be possible in the absence of any clinical information. However, there is zero PR depression which would be VERY unusual in pericarditis. P.S.: Acute pericarditis may produce diffuse ST elevation. Presence of STD is helpful; absence is not.
False Positive ST elevation in aVL Even when the story is obvious, with intractable pain, the STEMI paradigm can cause preventable delays Man in his 60's with very subtle ECG and pain not controlled with medical therapy Pericarditis vs. MI #2 See other "Quiz Posts": Quiz post - which of these, if any, are OMI? Will you activate the cath lab?
First, many on Twitter said "Pericarditis". This is NOT pericarditis, which virtually NEVER has ST depression any where except aVR. See our publication: ST depression in lead aVL differentiates inferior ST-elevation myocardial infarction from pericarditis There is STE in inferior leads, high lateral leads, and V4-V6.
In our hope of increasing appreciation of the clinical insights that this fascinating phenomenon may provide — we highlight its occurrence in our blog posts. I last reviewed the phenomenon of electrical alternans in My Comment at the bottom of the page in the November 28, 2022 post of Dr. Smith's ECG Blog.
PR depression, which suggests pericarditis 4. We also showed that, of 47 cases of pericarditis with ST elevation, none had ST depression in aVL. ) I’ll add the following 2 comments: i ) This patient presumably has effusive-constrictive pericarditis. Absence of any ST depression in aVL. ( Clin Cardiol 22:334-344, 1999 ).
This rules out pericarditis, which essentially never has reciprocal ST depression. This is not pericarditis because: a. Pericarditis does not have reciprocal depression. ST elevation of pericarditis is maximal in leads II and V5, V6. Pericarditis does not have hyperacute T-waves.
Of course the patient was saddled with the erroneous "pericarditis" diagnosis after CTs ruled also ruled out PE and dissection. The October 15, 2022 post in Dr. Smith's ECG Blog features no less than 20 ECG examples by Drs. Serial ECGs remained unchanged. But he did well.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." St depression in lead AVL differentiates inferior st-elevation myocardial infarction from pericarditis. The case continues. Worrall, C.,
Haven't you been taught that this favors pericarditis? Weren't you taught that concave morphology favors pericarditis? Expert ECG interpretation can often distinguish normal variant STE from OMI from pericarditis. Smith = “You diagnose acute pericarditis at your peril”. We will study this soon with our database.
Emre is a new Editor of the Blog. You can find many examples on this blog attesting that. I am sure that it is not for the readers of this blog. This is also a clear ECG for the readers of this blog, but may be hard for someone who is not used to seeing non-mainstream ECGs. Written by Emre Aslanger.
Echo does not necessarily differentiate acute MI from pericarditis: both may have wall motion abnormalities. Dr. Punjabi has a fantastic radiology blog on Spectral CT: [link] A negative CT should not be relied upon to rule out ischemia. This is why I frequently write: "You diagnose pericarditis at your peril."
ECG Diagnosis: Normal variant ST Elevation vs. Pericarditis. Uncertain whether there is pericarditis or normal variant. No objective signs of pericarditis (no rub, no effusion, no positional pain) 3. I favor normal variant for several reasons : 1. No active chest pain 2. Normal variant is far more common 4.
When there is MI extending all the way to the epicardium (transmural), that infarcted epicardium is often inflamed (postinfarction regional pericarditis, or PIRP). What complication is the patient with post-infarction regional pericarditis at risk for? 3) Oliva et al. (4) Lessons : 1. One should be on the alert for myocardial rupture.
We have seen this pattern in many pts with acute right heart strain on this blog. __ Smith : The combination of T-wave inversion in V1-V3 and in lead III is very specific for acute pulmonary embolism. Thus, the ECG could be considered similar to Aslanger's pattern (inferior OMI plus SEI pattern). What is the Diagnosis?
These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. Usually with pericarditis and myocarditis — hyperacute T waves (HATW) are not present. S mith : there is STE in lead III and reciprocal STD in aVL. This is OMI until proven otherwise.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of Chest Pain and Dyspnea Head On Motor Vehicle Collision. I've copied KEY points from My Comment in the August 6, 2022 post in Dr. Smith's ECG Blog — regarding the answer to this question.
Dyspnea, Chest pain, Tachypneic, Ill appearing: Bedside Cardiac Echo gives the Diagnosis 31 Year Old Male with RUQ Pain and a History of Pericarditis. Nicholson and Meyers provide numerous links at the end of their discussion to insightful related cases of acute PE that we've presented in Dr. Smith's ECG Blog. What is the Diagnosis?
It could also be due to pericarditis or myocarditis, but I always say that "you diagnose pericarditis at your peril." The clinical presentation is very suggestive of myo-pericarditis. But one should always remember that acute MI is a far more common pathology than myo- or pericarditis. Pericarditis? 13, 2019 Dr.
In this ECG Cases blog we look at 8 patients with potentially ischemic symptoms, to highlight pearls and pitfalls of inferior MI. Can you identify which ones had acute coronary occlusion? The post ECG Cases 3: Can you find the subtle inferior MI? appeared first on Emergency Medicine Cases.
In this ECG Cases blog we look at 10 patients who presented with ST elevation, and review the differential diagnosis of ST elevation using the ELEVATIONS mnemonic. Which had occlusion MI? The post ECG Cases 17 – ST ELEVATIONS mnemonic and Occlusion MI appeared first on Emergency Medicine Cases.
When there is MI extending all the way to the epicardium (transmural), that infarcted epicardium is often inflamed (postinfarction regional pericarditis, or PIRP). 3) strongly associated myocardial rupture with postinfarction regional pericarditis (PIRP) , and associated PIRP with persistent upright T-waves. 3) Oliva et al. (3)
In this ECG Cases blog we look at 10 cases of patients with chest pain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
Well, don't we see diffuse ST Elevation in Myo-pericarditis (with STD in aVR)? But it is very distinct from hyperkalemia (and anything else, including VT), and such confusion can only be due to lack of familiarity, because, if you look closely, its morpholgoy is very different from anything else. So this is STEMI, right? Which artery?
Fortunately, there was an ECG from about a year prior: And here is one from about 10 years prior: You can see here that the computer says "suggests pericarditis" but that I changed it to early repolarization. Just because there is diffuse ST elevation does NOT mean it is pericarditis. A picture is worth 1,000 words.
ST depression in lead AVL differentiates inferior ST-elevation myocardial infarction from pericarditis. Kontos et al. 2022 ACC expert consensus decision pathway on the evaluation and disposition of acute chest pain in the emergency department: a report of the American College of Cardiology solution set oversight committee. Bischof et al.
ECG 2 Especially in the context of the first ECG, readers of this blog will readily appreciate the ST elevations and hyperacute T waves in II, III, aVF, V6, and to a lesser extent V5. The "flu-like" illness suggests myo- or pericarditis, but that would be a diagnosis of exclusion. [link] I also texted the ECG to Dr. Smith.
Post-infarction Regional Pericarditis (PIRP) PIRP happens when MI is transmural, all the way from subendocardium to subepicardium, thus leading to inflammation of the subepicardium (next to the pericardium). MYOCARDIAL RUPTURE AND POSTINFARCTION REGIONAL PERICARDITIS KEY POINTS · Myocardial rupture occurs in 1 to 1.5% Re-occlusion 2.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content