This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
At their first appointment, the family met with a complete team of fetal and pediatric heart specialists, maternal fetal medicine experts, genetic counselors and other doctors to review and confirm Zanes diagnosis. Watch Zeke and Zanes story *This blog post is sponsored by the Heart Institute at Childrens Hospital Colorado.
citizen, national, or permanent resident; meet educational and credential requirements; and either be employed or begin training as a pediatric specialist at a PSLRP-approved site serving a medically underserved area or population. This program invests in current and future pediatric cardiothoracic surgeons to meet the growing demand.
The Pediatric Cardiology Certification Exam can be an overwhelming undertaking. The American Board of Pediatrics (ABP) provides detailed information about the pediatric cardiology certification exam, including the number of questions, sections, and the time allotted for each part. It won’t help you effectively study.
Transition/Lifelong Care Committee: Transitioning from pediatric to adult care can be a daunting journey. Education Committee: Knowledge is power, and this committee is dedicated to providing valuable resources and information to our community. From webinars to informative articles, they are committed to spreading awareness and understanding.
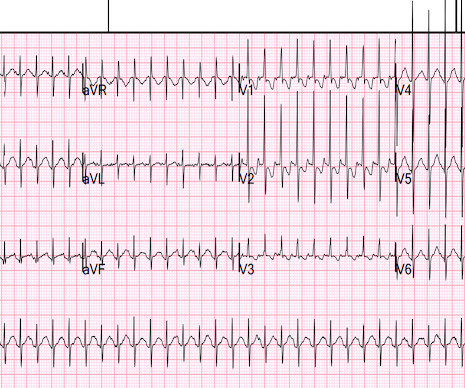
so it must be a pediatric ECG. This is typical of pediatric ECGs because the fetal circulation depends on the right ventricle. What can you say about this ECG at a rate of 230 beats per minute? Answer below The QRS is very narrow (about 70 ms?), Thus, what appear to be p-waves are indeed p-waves (see leads II and V1).
Previously, the education and resources on cardiometabolichealth.org were grouped only by format, such as CME courses, blogs, webinars, and expert interviews. For instance, a pediatric provider may be only interested in topics pertaining to childhood obesity.
Today, for the second blog of this series, Global Cardiac Surgery is featuring Guatemala, a lower-middle-income country in Central America serving as a hub and leading example for cardiac surgery in the Region.
This blog post aims to provide comprehensive information and support for families navigating the challenges of CHDs, offering insights into the medical, emotional, and practical aspects of managing this condition. It’s essential to work with a pediatric cardiologist who has experience with congenital heart defects.
The pediatric team felt it might be ACS, but on review of his prior ECGs, it was thought to be really unchanged from the 2 prior and more consistent with myocarditis. Dr. Punjabi has a fantastic radiology blog on Spectral CT: [link] A negative CT should not be relied upon to rule out ischemia. The troponin I returned at 9.3
It is important to remember that pediatric tracings manifest a number of differences from adult ECGs. Looking in the limb leads ( especially lead II , given the long R-R interval between the 2nd and 3rd beat in this lead ) — We would expect to see an extra P wave if there was 2:1 block.
He has a great blog too: ECG Interpretation He is also well known on the Facebook EKG Club page , where you can learn tons about ECGs: Here is his response, with the first ECG labelled: Hello Steve & Avinash. It is commonly seen in the reperfusion setting. It appears to be benign in children as well (see references below).
In this pediatric study, it was 71% successful and better than amiodarone. Meyers, Smith; Weingart wrote an extensive review on Idiopathic VT in the September 14, 2018 post of Dr. Smith’s ECG Blog. Procainamide is another reasonable solution to the problem. As a result — it’s worth briefly reviewing this entity of “ Idiopathic ” VT.
To create comprehensive reports, connect to applications dealing with 4D, echocardiography, nuclear medicine, CT angiography, and pediatric echo reporting. This is a great way to increase productivity in any medical setting.
A 6 yo girl had significant trauma from an MVC, with head injury (initial GCS 10, but no intracranial bleeding) and mild orthopedic injuries. She was intubated. A FAST exam was normal (no pericardial or peritoneal fluid). As part of her workup, this ECG was recorded: What do you think?
Learning points: == MY Comment , by K EN G RAUER, MD ( 1/15 /2024 ): == Today's case by Dr. Nossen differs from other cases of AV block we have published over the years in Dr. Smith's ECG Blog — in that the cause of AV block turned out to be CS ( C ardiac S arcoidosis ).
Pediatric and elderly patients were more predisposed to developing an arrhythmic event in the setting of fever [7]. Recently the rate of true arrhythmic events related to fevers in the classic Brugada Type 1 syndrome was explored by Michowitz et al. mm ( generally ≥2 mm ) in ≥1 right precordial lead, followed by a positive T-wave. —
Pediatric and elderly patients were more predisposed to developing an arrhythmic event in the setting of fever [7]. Recently the rate of true arrhythmic events related to fevers in the classic Brugada Type 1 syndrome was explored by Michowitz et al.
I've been working on this a long time, thought about submitting it to a journal, but decided it gets more readers on this blog. Instead, in this blog post we will compare the rule-of-thumb to each of the four formulas, effectively substituting usual care for the unattainable gold-standard of outcomes.
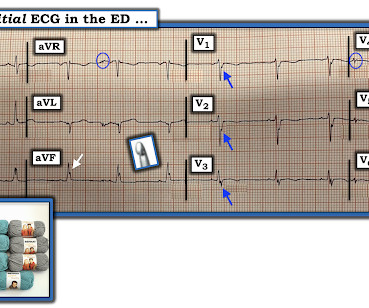
Acute coronary syndrome in a pediatric patient? An ECG was perfomed on arrival to our ED: NSR with ST elevation II,III, aVF with reciprocal depression in aVL Would you refer this pediatric patient for emergent PCI? World J Pediatr. The workup at the transferring hospital yielded elevated troponin I at 18.1 Epub 2021 May 20.
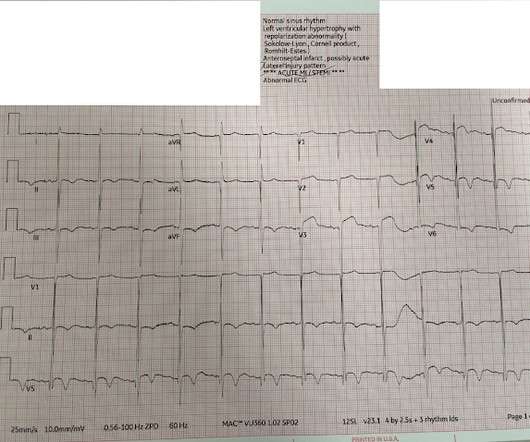
I suspect most blog readers did not struggle with this one. Toward this end we've conveniently added a LINK for "LVH Criteria" in the Menu at the top of every page in Dr. Smith's ECG Blog. I sent this ECG to Dr. Smith with no clinical context, and he immediately replied "Fake." Figure-1: I've labeled today's ECG.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content