This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
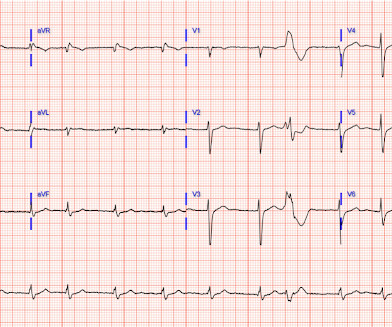
See ECG Blog #435 — ECG Blog #313 — as well as My Comment at the bottom of the page in the June 17, 2024 post in Dr. Smith's ECG Blog ). ECG Blog #233 — Reviews a case of Acute PE ( with discussion of ECG criteria for this diagnosis ). ECG Blog #119 — Reviews a case of Acute PE ( and ECG criteria for this diagnosis ).
Kayla and Misael sat outside our Cardiac Intensive Care Unit (CICU) facing a devastating diagnosis, when, like a scene from a movie, a nurse ran out to tell them they had found a heart donor. Numerous doctors, nurses, technicians and other specialists provided the clinical care that saved Zane and Zekes lives.
An old ECG was available, confirming this wide QRS is new and appears to be a dramatically widened version of his normal, narrow QRS: I stood up from my desk and asked our nurses to draw a VBG and place the patient on a monitor. As I did this, another nurse said, “room 19 is in V-tach!”
Before beginning this blog, I thought I would introduce you to the first two laws of regulation ‘ regulation-omics’ : I know that many of the things that are obliterating productivity in the NHS are happening in all health care services, everywhere. I think nurses have it worse than doctors. Nurses have no such freedoms.
Nurse notes: the silent scream of the heart The emergency nursing notes document the patient complaining of chest pain refractory to nitro, with a rising trop: 2200: ECG shown to ED MD 0020: repeat ECG shown to ED MD, patient complain of midsternal chest pain 0520: nitro x 3.
Within this group of 1206 professionals the following categories were use: Primary Care Physicians, Cardiology fellows in training, Resident physicians, medical students, advanced practice providers, nurses and allied health professionals. Plus a large group of non-physicians including nurses, physician assistants and nurse practitioners.
30th October 2022 [How fewer doctors means more doctors – it’s official] This blog has nothing to do with heart disease, or vaccines, or anything directly about medical practice at all. In the UK, more specifically England, doctors and nurses have been leaving the profession in droves. In particular GPs. Even GP numbers have increased!
The impact of these shortages has affected the gamut of healthcare worker roles -- from physicians and nurses to medical technicians and yes, radiologic technologists. House of Representatives Energy and Commerce Committee that deemed them a "national emergency." imaging market has an expected compound annual growth rate (CAGR) of 4.2%
As a nurse, I understand basic medical terminology. For example, it is okay to expect that the hospital has a dedicated CICU, with specialized CICU nurses. They went above and beyond to make me feel as comfortable as possible, while providing a realistic prognosis and expressing genuine concern for the well-being of my daughter.
She contacted her neighbor, a nurse, for help. We have shown that morphine is associated with worse outcomes (see learning points below) and have published many blog posts about it , such as this one: Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mass delusion (and Opiate pain relief). The case continues.
Blog Introducing New Technology to an Institution jbagley Wed, 03/02/2022 - 11:15 Innovation and new technology are essential to the progress of any specialty. Consistent Team In the operating room, it is important to develop a consistent team including nurses, anesthesiologists, physician assistants, and surgical assistants.
Watch Chris’ story *This blog post is sponsored by the Heart Institute at Children’s Hospital Colorado. These teams work together to coordinate a unique care plan for each patient, which adapts and evolves as children grow. Kay are trained and ready to ensure the best quality of life for those who began with the odds stacked against them.
Today, for the second blog of this series, Global Cardiac Surgery is featuring Guatemala, a lower-middle-income country in Central America serving as a hub and leading example for cardiac surgery in the Region. Since the establishment, over 1300 surgeries have been performed, with over 20,000 patients seen in the outpatient clinic.
Programs receive a set amount monthly from Medicare and Medicaid to provide nearly everything for people over 55 whose needs qualify them for a nursing home but who don’t want to enter one.
This blog post explores the development of such partnerships and their potential to transform healthcare outcomes. We can revolutionize patient care and significantly reduce cardiometabolic risk by fostering collaborative relationships and leveraging diverse expertise and experiences.
Thanks to one our great HCMC nurses, Ryan Burch. He figured this one out. A dialysis patient presented with dyspnea. He was a bit fluid overloaded and not hyperkalemic. This ECG was recorded: This was sent to me in a text that woke me from sleep, but not simultaneous with patient care.
Blog Giving Credit Matters. You should be giving credit to just about everyone you encounter: the medical student, resident, fellow, scrub tech, physician assistant, clinic nurse, respiratory therapist, pharmacist, research coordinator, office manager, parking attendant, cafeteria worker, IT help desk worker; you get the drift.
For patients without easy access, we work closely with family members, nurses, and medical assistants who can facilitate virtual visits. Back to blog Twitter Facebook Instagram Jana Goldberg, MD VP of Clinical Services & National Medical Director, Heartbeat Health Want to learn more?
My most talented blog readers are paramedics because they have to put themselves on the line every time they activate the cath lab. One of my most talented readers is a health care assistant (a nursing assistant) who has taken a keen interest in ECGs. And they teach me a lot. He can beat nearly anyone.
However, the triage nurse wrote a note saying that he did admit to chest pain yesterday, which he vaguely endorsed when questioned again. It was pointed out (using examples from this blog) that his ST elevation was morphologically more consistent with early repolarization, with ST/T ratio < 0.25 in V6 and J-point notching.
This program was unique because it placed nurses in hospitals to work with patients to create post discharge plans and reduce readmissions. Back to blog Twitter Facebook Instagram The post The Heartbeat in Conversation Interview Series, with Kristie Servais. We worked tirelessly to design and implement a program in record time.
The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiac arrest. Formula : There is not enough ST elevation in V2-V4 to be applying the LAD/early repol formula, but if it is applied, one gets 1.5 mm of STE at 60 ms after the J-point in lead V3, 400 ms QTc, and 6 mm of R-wave amplitude in V4.
Triage is backed up, and 10 minutes into your shift one of the ED nurses brings your several ECG s that has not been overread by a physician. Imagine you just started your ED shift. It's a busy Friday afternoon. All of the patients presented with chest pain , and they are all in triage.
At 0800 the cardiology fellow is called to the bedside by the nurse as the patient again complains about 4/10 chest pain. Firstly, we have shown on this blog that the ECG is not perfectly sensitive for OMI even in the best of hands. In Figure-1 I have excerpted from the above blog post, the Pearls of Wisdom from Drs.
Today, for the first blog of this series, Global Cardiac Surgery is featuring Ghana, a lower-middle-income country in West Africa with a strong history in the realms of cardiothoracic surgery.
So, we have to be able to work in teams in order to leverage the expertise of each of the team members, the nurses, and the medical assistants, technicians, as well as the cardiologists. Back to blog Twitter Facebook Instagram The post Welcome to the Heartbeat in Conversation Interview Series. appeared first on Heartbeat Health.
As I say to nurses, when some new ‘thing’ – which absolutely must be done – thuds onto their desk. If we assume that nurses are busy, and they sure are, you can’t simply squeeze extra stuff into their working day. But if it helps people with gambling then this is all fine, wonderful, super great? Or maybe not.
Choosing GEMMS ONE For Organizational Interoperability Healthcare leaders know that achieving ongoing and reliable organizational interoperability will take a lot of work.
This was sent by a reader: Dear Dr Smith, I am an EM resident and a rather new reader of your blog. Our triage nurse therefore ordered an ECG for him (which is standard in our dept for epigastric pain patients): What do you think? I am writing to ask for your opinion on an ECG one of my colleagues recently came across.
I was in the midst of writing another blog on what is wrong with the NHS, happily highlighting a few of the many pointless tasks that get in the way of clinical work. more nurses and health visitors, and 18.5% A nurse must also accompany you, to ensure that … what? 27th November 2023 Relentlessly falling productivity (Part a).
Although not expressly stated in the presentation here — I’ll assume that despite palpitations that awakened this nursing home patient + diaphoresis and some shortness of breath — that the patient was still hemodynamically stable — since Adenosine was given by EMS. PEARL #1 — Remember statistical likelihoods.
She had home health nurse visits, and a BMP was sent the next day (the day prior to admission, presumably after 120 mEq of KCl replacement -- if she was taking as directed). It would be difficult to get a nurse to give it faster! Hospital admission had been recommended, but she left that ED against medical advice. Is 40 mEq too much?
It had started just after nursing her newborn, about an hour prior, and she described it as a severe non-pleuritic “pressure” radiating to the back. This is written by Brooks Walsh. link] A 30 year-old woman was brought to the ED with chest pain. She had given birth a week ago, and she had similar chest pain during her labor.
During the resuscitation, I ordered 10 mEq KCl push, but the patient received 40 mEq of KCl, push (far more than recommended) The resident had ordered 40 mEq and that is what the nurses heard. Is 40 mEq too much? Or the right amount? Contrary to my expectations, after pushing 40 mEq, the K only went up to 4.2
Improved Provider Access Provider access refers to the ability of healthcare providers, such as physicians, nurses, and other medical professionals, to access relevant patient information, medical records, and clinical data within healthcare systems.
Finally she saw a cardiologist who confirmed that she did indeed have heart failure and needed to start some medications as soon as possible and he would arrange for a heart failure nurse to see her. How can you possibly build rapport and trust if you never see the same doctors/ nurses more than once?
This case reminds me of this 27 year old totally healthy nurse who was previously healthy, presented with acute pulmonary edema and the below ECG that is diagnostic of proximal LAD occlusion, and was dismissed because of her age. This gets drilled into them.
In spite of aggressive questioning, he denied chest pain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4. This 42 yo diabetic male presented with cough and foot pain.
This blog post aims to provide comprehensive information and support for families navigating the challenges of CHDs, offering insights into the medical, emotional, and practical aspects of managing this condition. Finding the Right Specialists : The first step in managing a CHD is finding the right medical team.
It would be difficult to get a nurse to give it faster! During the resuscitation, I ordered 10 mEq KCl push, but the patient received 40 mEq of KCl, push (far more than recommended) The resident had ordered 40 mEq and that is what the nurses heard. In the case presented, it is not clear to me that the 10 mEq of K was given rapidly.
There were GPs who simply refused to visit elderly residents in nursing homes. On my patch this was all GPs and all nursing homes. Here is a section from a blog I wrote in March 2020. I worked with doctors who strode around the wards in positive pressure protective gear. It is one of the few satisfactions I get in life nowadays.
It’s an intubated septic nursing home patient." I received this ECG in a text message, with the message: "Hey, these look like hyperacute T waves to me, what do you think? Here is her old ECG:" What do you think? Here is my response: "There is something wrong with this ECG. It might be another case of pulse tapping artifact.
In the evening, a middle-aged man complained of chest pain at the nursing home. Nurses found him with a BP of 50/30 and heart rate of 130 and called EMS. He was awake, with a pulse of 130 and BP of 50/30. Fluids were started. The patient arrived alert but cool and clammy. His chest pain was vague. He complained of chronic dyspnea.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Expert commentary provided by Dr. Ken Grauer CASE 1 An 82 y/o Male called 911 for sudden onset dizziness while at rest. Upon arrival he was found alert and oriented, and without gross distress. He denied difficulty breathing, epigastric pain, or chest discomfort.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content