This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ECG in Figure-1 — was obtained from a middle-aged woman with positional tachycardia and diaphoresis with change of position from suprine to sitting. My THOUGHTS on the ECG in Figure-1: The rhythm is sinus tachycardia at ~105/minute ( ie, The R-R interval is regular — and just under 3 large boxes in duration ).
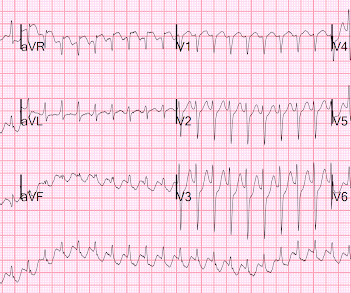
IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made. As discussed in ECG Blog #231 — Bidirectional VT is a special form of VT, in which there is beat-to-beat alternation of the QRS axis.
Voltage for LVH is satisfied — at least by Peguero Criteria ( Sum of deepest S in any chest lead + S in V4 ≥23 mm in a woman — as discussed in ECG Blog #73 ). This point is particularly relevant regarding ECG #2 — because sinus tachycardia is seen on this earlier ECG. Smith's ECG Blog — Drs. NOTE: It's EASY to get fooled by LVH!
With experience, applying the P s, Q s, 3 R Approach ( See ECG Blog #185 ) — to formulate the above steps in our initial assessment of the rhythm in Figure-1 can ( should ) be completed in less than 30 seconds! These are reviewed in ECG Blog #343. What about the 1 2- L ead E CG ? The QTc is not overly prolonged.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Are you confident there is no ischemia? Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Is this: 1.
It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. Even with tachycardia and a paced QRS duration of ~0.16
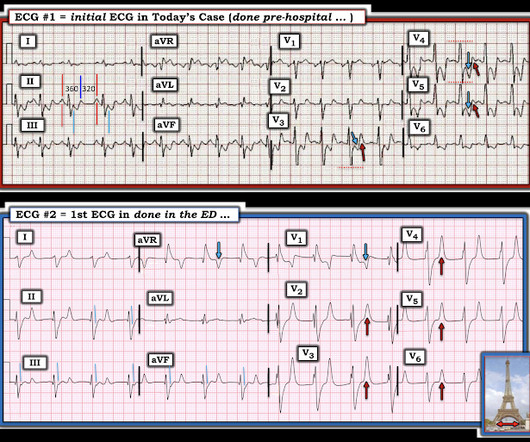
MY Interpretation of Today's Initial ECG: I've labeled key findings in Figure-2 for today's initial ECG: The rhythm is sinus tachycardia at ~105/minute. The sinus tachycardia is a definite concern that something acute may be ongoing. Does the patient's age infuence your interpretation? Figure-1: The initial ECG in today's case. (
ischemia) or it can be secondary to abnormal depolarization (e.g Discussion: The ECG in today's case does not have typical ST depression vector of diffuse subendocardial ischemia. The ST vector in subendocardial ischemia (SEI) usually has the largest amount of ST depression in leads II and V5, towards the apex of the heart. (ST
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. The patient was brought to the ED and had this ECG recorded: What do you think? And what do you want to do?
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
The terminology favored to describe these ECG findings is diffuse subendocardial ischemia ( See ECG Blog #271 — for more on diffuse subendocardial ischemia ). Smith’s 8/9/2019 post in his ECG Blog. R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation.
By the P s, Q s, 3 R Approach ( as reviewed in ECG Blog #185 ): The Q RS complex is obviously wide. Given the rapid rate of the tachycardia and the amorphous shape of the QRS — the decision was made to sedate the patient and cardiovert. ECG Blog #185 — Systematic P s, Q s, 3 R Approach to Rhythm Interpretation.
The Long Lead II Rhythm Strip: As always — I favor a systematic approach to rhythm interpretation, using the P s, Q s, 3 R memory aid ( See ECG Blog #185 ). The other main consideration — is to take another look at the 12-lead ECG, and assess this for recent ischemia or infarction.
PEARL # 6: As I discuss in my review of SSS ( See ECG Blog #342 for details ) — establishing a diagnosis that sinus bradycardia indicates SSS — will depend on the following: Finding out the age of the patient ( ie, SSS is most common in older individuals ) — and learning whether the patient has been symptomatic? No pause beyond 2.0
The finding of a fairly regular, wide tachycardia without clear sign of atrial activity ( especially when seen in an acutely symptomatic patient ) — should immediately prompt a diagnosis of VT until proven otherwise. Shark Fin" ST segment elevation is most often a sign of severe transmural ischemia that results from acute coronary occlusion.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). During the next 24 hours, she experienced periods of complete AV block with a ventricular escape rhythm in the 20s.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
This is ischemic ST depression, and could be due to increasing tachycardia, with a heart rate over 130, but that is unlikely given that the patient is now complaining of crushing chest pain and that there was tachycardia all along. They agreed ischemia was likely in the setting of demand given DKA and infection.
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. 2) Tachycardia to this degree can cause ST segment changes in several ways. Again, not an expected outcome with diltiazem).
ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management Cardiac Arrest.
It is a regular narrow complex tachycardia. There is a lot of ST depression -- this is ischemia caused by the very fast rate and is an indication for emergent electrical cardioversion. Ischemia is gone. Regular Narrow complex tachycardia, if not sinus tach, is AVNRT, AVRT, or atrial flutter with 1:1 or 2:1 conduction.
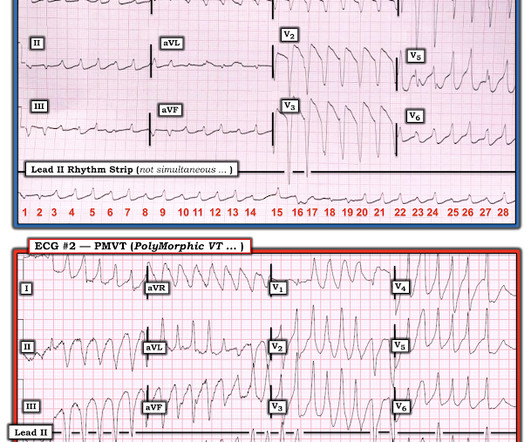
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). There is no definite evidence of acute ischemia. (ie, Some residual ischemia in the infarct border might still be present.
While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. Additionally, the qR morphology, particularly in a patient with right bundle branch block (RBBB) type wide QRS complex tachycardia (WQCT), lends further support for VT. What is the rhythm?
Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? She had a very elevated troponin T at 12,335 ng/L at the time of presentation. The patient in today’s case suddenly became tachycardic while sleeping.
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock. He had this ECG recorded. Are the lungs clear?
Here is his initial rhythm strip (it is not a full 10 seconds): Wide complex tachycardia, rate 235 This is a very wide complex regular tachycardia at a rate of 235. It should be considered to be Ventricular Tachycardia and treated as such. He was pale and diaphoretic (in shock) with a thready radial pulse. So what happened?
Here is his ECG: Original image, suboptimal quality Quality improved with PM Cardio digitization The ECG is highly suggestive of acute right heart strain, with sinus tachycardia, S1Q3T3, and T wave inversions in anterior and inferior with morphology consistent with acute right heart strain. Moreover, there is tachycardia.
With normal EF the tachycardia is not compensatory. The same reciprocal relationship is seen in severe subendocardial ischemia, just with opposite vector direction where V1 can show ST elevation) Below you can find the 3D model of the heart and coronary vessels. And the patient has sinus tachycardia. ( HR about 90-100/min.
The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia. Polymorphic ventricular tachycardia can be ischemic, catecholaminergic or related to QT prolongation. Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. Acute ischemia?
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ). Sinus Tachycardia ( common in any trauma patient. ).
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
An EKG was repeated around midnight: By itself, this ECG is not diagnostic of anything besides sinus tachycardia, and could be called normal (although there is ST segment straightening in the anterior leads, which should always prompt suspicion). The conventional computer algorithm called “ sinus tachycardia, otherwise normal EKG ”.
There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). This patient was having recurrent episodes of polymorphic ventricular tachycardia with an underlying long QT interval ( = Torsades des Pointes ). ECG #2 Interpretation of ECG #2: Underlying sinus rhythm.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This rules out subendocardial ischemia and is diagnostic of posterior OMI. V4-5 continue to show STD.
When PMVT is associated with a long QT interval — the rhythm is then defined as Torsades de Pointes ( Please SEE My Comment at the bottom of the April 29, 2020 post in Dr. Smith’s ECG Blog ). Figure-3: Comparison of ECG #1 with an example of PMVT, that I took from the October 12, 2013 post from Dr. Smith’s ECG Blog ( See text ).
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. I said I think there is a fixed stenosis in the LAD and the tachycardia and stress caused a type 2 STEMI.
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
Here is the only prehospital 12-lead: Sinus tachycardia, somewhat wide QRS, Ischemia Here is the first ED ECG: What is the rhythm here? Medics found patient in PEA arrest. He was resuscitated into a perfusing rhythm. He went in and out of arrest until arrival at the ED.
This proves effective treatment of the recurrent ischemia. The patient had no further symptoms of ischemia. EKG 3 is diagnostic for developing re-occlusion, and EKG 4 proves that the nitrates relieved the ischemia. = This proves effective treatment of the recurrent ischemia." Here was her final EKG prior to discharge.
We have also shown several cases in which atrial flutter hides true, active ischemia. Tachycardia and ST Elevation. Tachycardia to this degree can cause ST segment changes in several ways. Tachycardia to this degree can cause ST segment changes in several ways. Christmas Eve Special Gift!! Is this inferor STEMI?
Tachycardia and ST Elevation. == MY Comment , by K EN G RAUER, MD ( 7/7 /2024 ): == Among the most rewarding type of case for me during my days working in the ED — would be seeing a patient who presented with acute CP ( C hest P ain ) — who I would be able to “cure” simply by recognizing and treating their arrhythmia. Would you give lytics?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content