This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This confirms that the pain was ischemia and is now resovled. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The i nitial hs troponin I returned 75%.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. This EKG is diagnostic of transmural ischemia of the inferior wall. Edited by Smith He also sent me this great case.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished.
This suggests further severe ischemia. MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. And yet the arteries remain open.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
This was interpreted by the treating clinicians as not showing any evidence of ischemia. His ECG at the accepting facility is shown below: Accepting facility ECG The team reviewed his angiography films with an interventionalist and thought they were suspicious for plaque rupture in LAD, but they were not confident.
This proves effective treatment of the recurrent ischemia. The patient had no further symptoms of ischemia. Learning Points: Type 1 MI is the type we are most familiar with: rupture of atherosclerotic plaque with production thrombus or platelet fibrin aggregates. This proves effective treatment of the recurrent ischemia."
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. Ischemia can be disguised by a wide escape rhythm, which decreases the sensitivity of ECG.
This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. If there is also subendocardial ischemia, the ST depression vector remains leftward, with a reciprocal ST Elevation vector also to the right.
Although radiation into the left arm is most classic for coronary ischemia, radiation into both arms is actually modestly more predictive ). The primary care physician's note indicates low suspicion for cardiac ischemia, but "for completion, check troponin and ECG." If an ECG was obtained in the office, it was not saved. < 0.033).
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
The precordial STD persists in severity from V4-V6, rather than being maximal in V1-V4 (as in posterior OMI), and so the ECG overall best fits the subendocardial ischemia pattern (diffuse supply/demand mismatch). Meyers serves as a reminder of the important clinical entity known as diffuse subendocardial ischemia.
Time 17 minutes Not much different One month earlier This is Left Bundle Branch Block (LBBB) without any sign of ischemia. Ramus: There is a large caliber branching ramus intermediate LAD is a medium caliber vessel that extends to the apex and is noted to have diffuse mild to moderate plaque in the midsegment. Post Procedure TIMI III.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
She is diagnosed with "demand ischemia" and discharged home. (#2) She had the following EKG at 0700 : (#3) Here there is 4 mm of ST elevation that can only be due to myocardial ischemia. There was a ruptured plaque with thrombus in the LAD, with some flow still (accounting for the inverted T waves). Echo the next day is normal.
To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! One of the most common is rupture of a non-obstructive plaque, with thrombus formation and OMI that spontaneously lyses and leaves a wide open artery. It can only be seen by IVUS.
In this blog, we’ll break down the steps of coronary circulation, helping you understand how your heart maintains its own health while keeping the rest of the body alive and well. This is where coronary circulation comes into play. CAD is one of the leading causes of heart attacks.
Today, they viewed the angiogram and concluded that the thrombus at the mid RCA must have extended proximally from the culprit ruptured plaque, extending proximal to the RV marginal branch and temporarily occluding it. See P.S. below ) == P.S. : I believe I found another example of ischemia-induced J waves ( See Oct.
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. The rhythm is atrial fibrillation. The QRS complex is within normal limits. These include.
Smith comment: T-wave inversion such as seen in the first ECG can be seen with active non-transmural ischemia. But in this case, it is due to active ischemia, resolves with resolution of ischemia, and has little if any troponin elevation. If this patient was discharged from the ED she very likely would have died.
Is this Acute Ischemia? Reperfusion of OMI indicates at least partial thrombolysis of occluding thrombus, but still unstable plaque rupture, which can reocclude at any moment. No formal echo was done, and EF was normal on ventriculogram during cath, with no obvious wall motion abnormalities. More on LVH. LVH with anterior ST Elevation.
The septum appears a bit darker than the rest, and you might be fooled into thinking there is ongoing ischemia here. Dr. Punjabi has a fantastic radiology blog on Spectral CT: [link] A negative CT should not be relied upon to rule out ischemia. See an examples of CT ischemia here. Another troponin returned at 23.89
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. As there was ruptured plaque, this is NOT Prinzmetal's angina. Values: STE60V3 = 2.0, There was good flow.
This strongly suggests reperfusing RCA ischemia. Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found.
T-wave inversion in V2 is inconsistent with early repol, and is typical of posterior ischemia. In addition, there is ST depression, diagnostic of ischemia, in V3-V6. Nevertheless, even young people have atherosclerosis and plaque rupture. T-waves in inferior leads are hyperacute, out of proportion to those in early repol 5.
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point. Again, cath lab was not activated. What does this troponin level mean?
These are therefore not looking for coronary disease but instead ischemia heart disease. Remember functional tests tell you about ischemia and anatomical tests tell you about coronary disease. It is still possible to have ischemia without coronary disease. The problem with CT scanning is if you see something.
Only after her troponin peaked at 500,000 ng/L did she get her angiogram, which showed a 100% left main occlusion due to ruptured plaque. Young people can suffer acute coronary occlusion, whether by typical atherosclerotic plaque rupture, or by coronary anomalies, coronary aneurysms, dissections, spasm, etc. Diagnostic of Massive OMI.
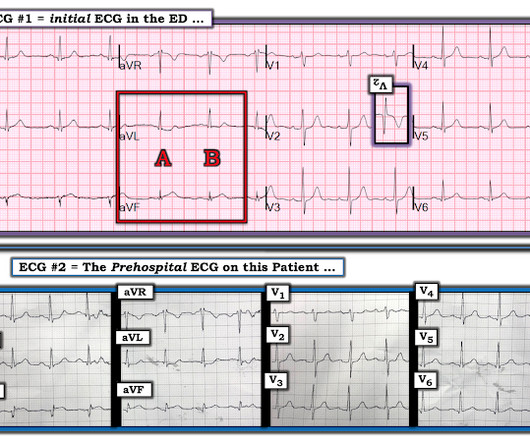
[link] Case continued: In this case, the diagnosis was much easier because there was a prehospital ECG: less than 1 mm ST Elevation in II, III, aVF, with minimal ST depression in aVL This is diagnostic of inferior OMI No clear evidence of ischemia Computer interpretation Impressive! This algorithm called it a STEMI.
Angiogram --Minimal coronary atherosclerosis --No obstructive epicardial coronary artery disease or evidence of plaque rupture noted to explain prolonged QT or ventricular fibrillation cardiacarrest, suspect nonischemic mechanism Echo The estimated left ventricular ejection fraction is 45 %. Acute ischemia? Use of QT-prolonging drugs?
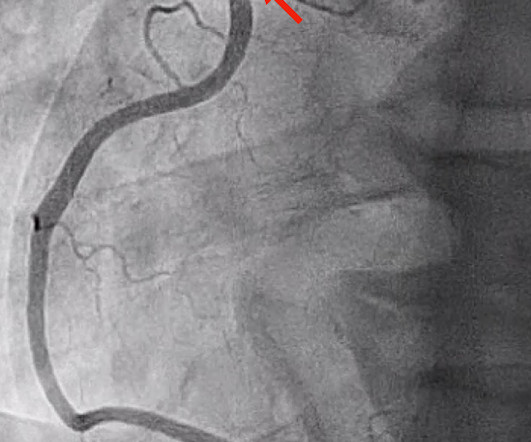
RCA ischemia often results in sinus bradycardia from vagal reflex or ischemia of the sinus node. He was taken to the cath lab and underwent emergent intervention: Thrombotic stenosis of the proximal RCA (95% with evidence of plaque rupture) is the culprit for the patient's inferoposterior STEMI. He was successfully stented.
Even though this blog is devoted to understanding the nuances of EKG, we always need to remember that an EKG is only a single test. The operator performed intravascular ultrasound and visualized acute plaque rupture with thrombus formation and placed a stent. There was reperfusion ischemia superimposed on benign T-wave inversion.
But it also shows a massive area of total ischemia in the LAD territory: CT shows the infarct The CT is with contrast, which increases density (which looks more white). This was ruptured plaque with thrombus. Most dissections which cause coronary ischemia are into the RCA ostium ("ostium" = locations of takeoff of the vessel).
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Mechanisms of plaque formation and rupture. Coronary plaque disruption. Journal of Geriatric Cardiology , 19 (6).
Time 7 hours lead reversal There is limb lead reversal (QRS in I and aVL are now inverted), but nevertheless one can see that the ischemia appears to have resolved. This was attributed to a "Type 2 MI", which is acute MI that is not due to ruptured plaque, but rather due to "supply demand oxygen mismatch". Next day, with K = 4.6
That said there were no clinical symptoms or ECG findings suggestive of ongoing ischemia. The intricacies of the different classes of antiarrhythmics and their mechanism of action extend beyond the scope of this blog. There were no plaques or stenoses. I list below links to other cases of idiopathic VT from Dr Smith's ECG blog.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content