This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ECG does not show any definite signs of ischemia. IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ).
There may be ischemia present, but it is not evident on the ECG. In this paper, Dr. Birnbaum writes: "In patients with ACS without LVH, ST depression with negative T waves in the lateral leads is a sign of sub-endocardial ischemia and is an independent predictor of adverse outcome [11 – 13].
Readers of this blog can easily appreciate the hyperacute T waves in the precordium, clearest in V1-V4. In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. the investigators reviewed outcomes in 118 patients presenting with NSTEMI.
But it was interpreted as no acute ischemia and the patient was referred to cardiology as Non-STEMI. Cardiology: delayed cath = Non-STEMI Heres the interventional cardiology note describing the ECGs, management and outcome: He has had transitory peak T-waves, ST-segment elevation, and biphasic T-waves during recurrences of pain.
The patient with no prior cardiac history presented in the middle of the night with acute chest pain, and had this ECG recorded during active pain: I did not see any ischemia on this electrocardiogram. The patient has active chest pain, so if these are abnormally large T-waves This link shows 13 blog posts of Posterior Reperfusion T-waves.
The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia. Regular readers of this ECG Blog will be well familiar with many of these points. For more on use of Opiates with acute ischemic CP — See the January 6, 2023 post in Dr. Smith's ECG Blog ).
The first ECG was labeled “anterior subendocardial ischemia”, but subendocardial ischemia does not localize. If there were diffuse ischemic STD, with precordial STDmaxV5-6 and reciprocal STE-aVR, this would be non-specific subendocardial ischemia from ACS or supply-demand mismatch.
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. Finally, head-up CPR (which was not used here), makes for better resuscitation.
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Brief aside: "Early repolarization" is a frequently proclaimed and poorly understood electrocardiographic phenomenon which mostly serves to reassure clinicians that not all ST elevations are ischemic (something readers of this blog know well).
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
When the ischemia is resolved, if there is no infarction, the T-wave can normalize. When I see a case like this, I am skeptical that the ECG is manifesting acute ischemia or reperfused OMI. Outcome: All hs troponin I ﹤ 3 ng/L (undetectable). On occasion, unstable angina can present with reversible T-wave inversion during pain.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
My most talented blog readers are paramedics because they have to put themselves on the line every time they activate the cath lab. Outcome and Analysis: ECG 1 is diagnostic of inferior and right ventricular MI. The minute this medical student saw the first ECG, he knew the diagnosis without any further information. right ventricular?
If this STD were due to LVH or to subendocardial ischemia, rather than posterior OMI, it would be maximal in V5 and V6. If I saw this without the STD V2-V4, I would not make anything of it, and even with that precordial STD, I am not convinced that it is a manifestation of ischemia. Alcohol intoxication? V5-V6), even if less than 0.1
1-3] But these studies were very short duration and used cardiology interpretation of ECGs or emergent angiography rather than patient outcomes. Dr. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al. Acad Emerg Med.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
What was the outcome?" There is akinesis of the distal septum, anterior, apex, and distal inferior wall consistent with LAD territory ischemia or infarction. This was sent to me without any info while I was out and about, and I looked at it on my phone. I responded: "That is a tough one. V2 is very worrisome. But no other leads are.
We have also shown several cases in which atrial flutter hides true, active ischemia. Long-term outcome is unknown. First, there can simply be diffuse STD (which obligates reciprocal STE in aVR) associated with tachycardia, which are not even necessarily indicative of ischemia. Christmas Eve Special Gift!! Is this inferor STEMI?
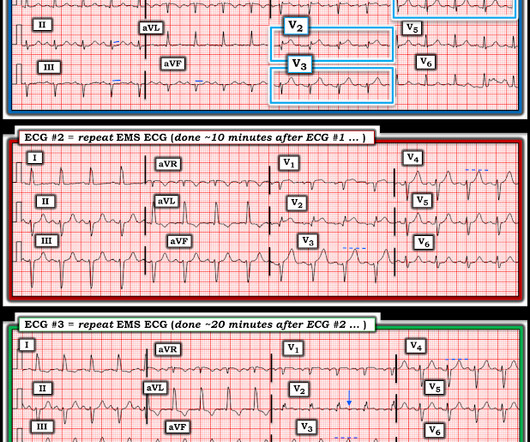
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
But ECGs interpretation is often conflated with clinical assessment, so if patients don’t present with chest pain the ischemic changes are not seen or are attributed to something other than ischemia. Instead, ECGs need to be interpreted in isolation and then applied to the patient.
Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Acute ischemia? Case continued The tachyarrhythmia terminated on its own. Use of QT-prolonging drugs?
2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. The absence of STE in V7-V9 is often due to resolution of ischemia, as seen by resolution of ST depression in V7-V9. non-occlusive ischemia) JAHA 2021 3. -- Meyers HP, Bracey A, Lee D, et al.
For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. I have seen cases of Wellens' syndrome that were ignored because of either negative troponins or normal echo or both and the patient did not get an angiogram and had a bad outcome. Wellen's syndrome is a Reperfusion syndrome.
Groups were categorized based on moderate to severe chest pain (numerical rating scale pain ≥ 5/10) or less than moderate severity to compare procedural and clinical outcomes. And as we have shown before, morphine leads to slower times to treatment and worse outcomes. 414 patients were included in the analysis.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). I've copied KEY points from My Comment in the August 6, 2022 post in Dr. Smith's ECG Blog — regarding the answer to this question.
Outcome of case 2? In addition — there is transmural ischemia of the septum , most often resulting from occlusion proximal to the 1st septal perforator branch of the LAD. This one, too, is a swirl pattern and diagnostic of LAD occlusion. Admitted for NSTEMI. Cath days later showed complete occlusion of the LAD, stented.
There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). Opiates are associated with worse outcomes in Myocardial Infarction. It is one of the few OMI patterns that is really well described: de Winter’s T-waves. Am Heart J.
There is about 1 mm of STE in aVR I con sidered but rejected subendocardial ischemia. Is it subendocardial ischemia, or inferior MI? Outcome : Was it RCA or LCX with inferior MI? The ST elevation vector is posterior, inferior, and right , to the right of lead III and also posterior.
Answer : There is very abnormal T-wave inversion in aVL which is typical of subtle transmural/subepicardial (due to occlusion) ischemia to the inferior wall. Similarly, the precordial T-wave inversions in V2-V4 are reciprocal to posterior wall transmural/subepicardial (due to occlusion) ischemia. This is reciprocal T-wave inversion.
Smith : the profound persistent STE suggests either persistent occlusion or " no reflow " with persistent downstream ischemia. Long term outcome unknown but obviously bleak. It makes you think you have done something for the ischemia when you have not! In the first year since discharge, he has been hospitalized 3 times with CHF.
Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer: This is a posterolateral MI. Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. This ECG is diagnostic of ischemia. Is this due to coronary occlusion?
None of these findings are diagnostic of ischemia, but they should give you a high index of suspicion and prompt serial ECGs at a minimum. He underwent PCI and had a good outcome. Ischemia comes and goes. mm of STE at 60 ms after the J-point in lead V3, 400 ms QTc, and 6 mm of R-wave amplitude in V4. Learning Points: 1.
This suggests further severe ischemia. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. Detailed coronary artery evaluation not performed. Exam was interpreted and discussed with Dr. Simegn of cardiology, who reviewed the cardiac portion.
Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. But the real question at hand is: Are these precordial ST-depressions a result of subendocardial ischemia?
Outcome: Patient ruled out for MI by troponins. And ECGs can change and evolve even when there is no ischemia. Wang and Smith as suggestive of BTWI ( These criteria were cited by Dr. Meyers in the March 22, 2022 post of Dr. Smith's ECG Blog ). Here is a great case of pseudonormalization. Here are multiple cases. in ECG #1 ).
I do not think this ECG is by itself diagnostic of OMI (full thickness, subepicardial ischemia ), b ut comparison to a previous might reveal this ECG as diagnostic of OMI. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. Abstract 556.
Here is a link to a blog post with the formula , which we have recently validated and will publish. After the hyperacute phase, the ST segments rise and only fall with either 1) reperfusion or 2) prolonged ischemia leading to irreversible infarction. As for thrombolytics, that is a bit riskier. 3.0 = 0.50 The height of the ST segments.
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." When the ischemia is resolved, the wall motion may completely recover, or there may be persistent stunning.
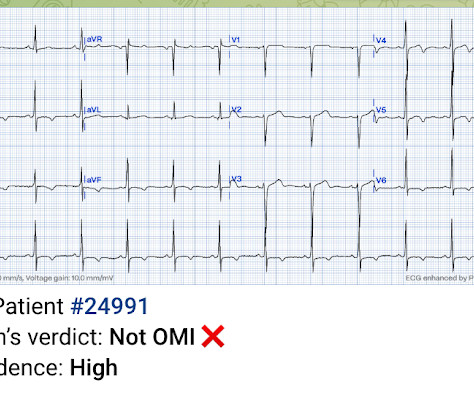
Here is PM Cardio's Queen of Hearts interpretation (AI ECG interpretation trained by Meyers, Smith, and PM Cardio team using thousands of cases and their outcomes): The output number ranges from 0 to 1, with numbers closer to zero meaning likely NOT OMI, and numbers closer to 1 meaning OMI.
The patient survived with unknown long term outcome. Instead — QRS widening is almost certainly related to acute ischemia from extensive infarction, thereby suggesting another adverse prognostic factor. No further ECGs were recorded. She was very lucky to have spontaneous reperfusion.
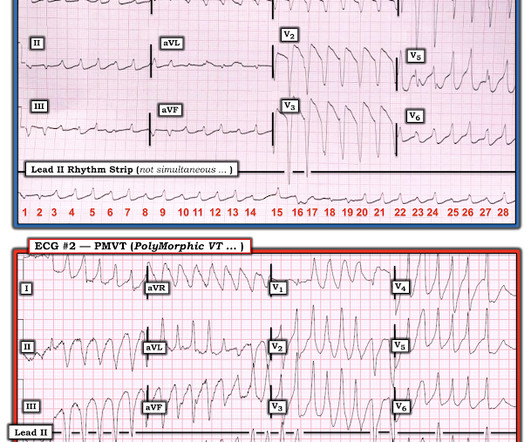
When PMVT is associated with a long QT interval — the rhythm is then defined as Torsades de Pointes ( Please SEE My Comment at the bottom of the April 29, 2020 post in Dr. Smith’s ECG Blog ). Figure-3: Comparison of ECG #1 with an example of PMVT, that I took from the October 12, 2013 post from Dr. Smith’s ECG Blog ( See text ).
All of this appears to be consistent with "No Reflow", or small vessel occlusion with persistent ischemia in spite of an open artery. Thus, this ECG predicts poor myocardial perfusion and poor outcome. Small vessel occlusion is measured by "blush" on the angiogram, and codified by TIMI Myocardial Perfusion (TMP) Grading.
There is normal R-wave progression in the precordial leads with no evidence of ischemia. Here the image quality is enhanced using the PM Cardio app. What do you think? The presenting ECG shows SR with narrow QRS complexes. In the limb leads there is T-wave inversion in lead aVL with a low amplitude QRS preceding the T-wave.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content