This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
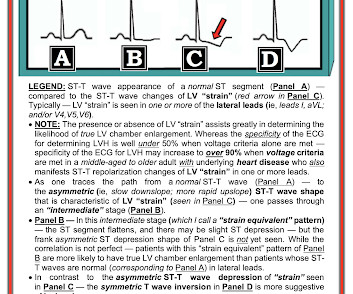
This leaves us with the usual differential diagnosis for this rhythm presentation ( as per ECG Blog #361 ) ==> We need to consider i ) VT until proven otherwise: ii ) SVT with either preexisting BBB or aberrant conduction; — or , iii ) Something else ( ie, WPW, hyperkalemia, some other toxicity, etc. ). What Kind of Conduction Defect?
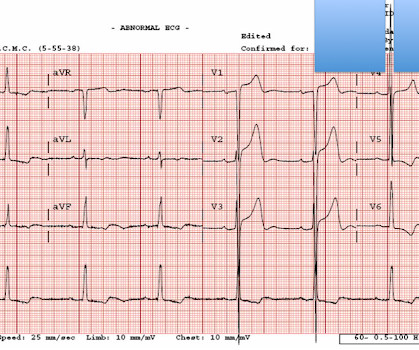
The ECG in Figure-1 was obtained from a middle-aged man with known hypertension — who presented to the ED ( E mergency D epartment ) for CP ( C hest P ain ) over the preceding 2-3 days. For more regarding ECG criteria for LVH — See the ADDENDUM below and/or ECG Blog #73 and ECG Blog #245. Should you activate the cath lab?
NOTE: For more on ECG recognition of RVH and/or pulmonary hypertension ( re the qR pattern in lead V1 ) — See ECG Blog #234 and Blog #248. This could have been an optimal time to try a Lewis Lead — which sometimes reveals atrial activity not evident with standard lead placement ( See ECG Blog #223 ).
The ECG in Figure-1 was obtained from a middle-aged woman — who presented with low back pain, shortness of breath and marked hypertension — but no CP ( C hest P ain ). Today's patient is a middle-aged woman who presented with low back pain, shortness of breath and marked hypertension — but no chest pain. The KEY lies in the history.
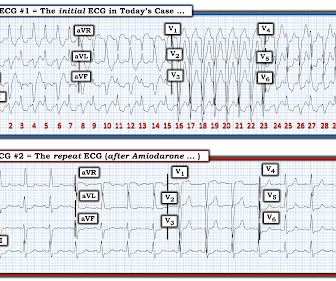
== P lease N OTE : After today — No new ECG Blog posts for 2- to -3 weeks. — I will also not be prompt in replying to emails. == All material on this ECG Blog site remains open! IF you scroll down a little on the right-hand column of this blog — You'll see a lot of icons. Figure-1: The initial ECG in today's case.
She had a history of hypertension, and was on medication for this — but she was otherwise healthy. Contrast today's rhythm with true ventricular bigeminy — that was seen in ECG Blog #343 ). Contrast today's rhythm with true alternating bundle branch block — that was seen in ECG Blog #306 ). Is this Ventricular Bigeminy?
In this ECG Cases blog we look at 10 patients with shortness of breath, and discuss how the ECG can be used to help diagnose cardiac, respiratory and metabolic emergencies. For RV strain, acute vs chronic, we should look for signs of acute RV strain and chronic pulmonary hypertension.
An undergraduate (not yet in medical school) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly arrived at work and happened to glance down and see this previously recorded ECG on a table in the ED. It was recorded at 0530: What do you think?
He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder. Written by Magnus Nossen The patient in todays case is a 50 year old male. The patient presented due to chest pain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chest pain.
These cases are particularly challenging because traditional prevention strategies, which target known risks like high LDL cholesterol, hypertension, diabetes, and smoking, may not apply. Stay tuned for our next blog, where we’ll outline actionable solutions to make prevention more effective and accessible.
Bakris , an internationally recognized and influential nephrologist and hypertension expert, who passed away on June 15, 2024, at the age of 72. This week’s blog celebrates the life and legacy of Dr. Bakris. A Pioneering Journey: The Life and Legacy of Dr. Bakris Dr. George L.
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the Emergency Department for acute chest pain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. Vitals were within normal limits except some hypertension. Which is true.
Written by Willy Frick with edits by Ken Grauer A woman in her 70s with a history of hypertension presented with acute onset shortness of breath. ECG Findings of Acute PE in Today's Case: We periodically highlight cases of acute PE ( See the June 17, 2024 post in Dr. Smith's ECG Blog — that includes links to over 25 of these cases ).
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Before beginning this blog, I thought I would introduce you to the first two laws of regulation ‘ regulation-omics’ : I know that many of the things that are obliterating productivity in the NHS are happening in all health care services, everywhere. But this, the primary guideline on hypertension for adults, is but one of many.
In this CritCases blog - a collaboration between STARS Air Ambulance Service, Mike Betzner and EM Cases, we take you through a not uncommon stroke presentation which then develops into a challenge with regard to management of elevated ICP, hypertension and the airway.
Furthermore, the patient has no chest pain (certainly many STEMI do not have chest pain, but it should always make you especially scrutinize the ECG and the clinical situation) and there was severe hypertension. The hypertension alone is the likely etiology of the pulmonary edema. The cath lab was activated.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. Regular readers of this ECG Blog will be well familiar with many of these points.
This blog explores how genetics influence heart health and whether mitigating these inherited risks is possible. Maintain a Healthy Weight: Obesity amplifies the effects of genetic predispositions by contributing to high cholesterol, hypertension, and diabetes.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. Back to the case.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chest pain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. It is a ssociated with mild dyspnea on exertion. At times the pain does go to his left neck.
Seen together, these 2 ECG findings suggest possible RVH ( For review on "My Take" for the ECG diagnosis of RVH — Please see My Comment at the bottom of the page in the March 6, 2022 post and in the September 1, 2020 post of Dr. Smith's ECG Blog ). There is no reciprocal ST depression.
This blog explores the ways wearable technology can help track heart health, the advantages it offers, and how it contributes to better outcomes for those requiring surgical intervention. By understanding patterns in heart rate, blood pressure, and oxygen levels, surgeons can tailor procedures to the individuals needs.
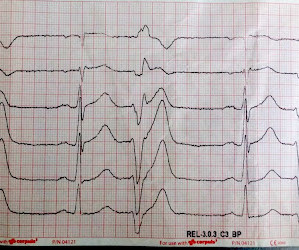
TCP in the ROSC Patient: False Electrical Capture at 75mA Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the second installment of a blog series showing how transcutaneous pacing (TCP) can be difficult and how you can improve your skills. Epinephrine administered intravenously.
In this week’s CMHC Pulse Blog Post, Virend K. There is a clear relationship between sleep deprivation and the development of conditions like obesity, diabetes, and hypertension. As healthcare providers, it’s crucial to understand the profound connection between sleep disorders and cardiometabolic health.
Another possible cause of pseudonormalization of T waves mentioned many times on this blog is the pseudonormalization caused by re-occlusion of an infarct related reperfused coronary artery. A VSR is more likely to occur in patients who are older, female, hypertensive, have chronic kidney disease, and have no prior history of smoking.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. From My Comment in the November 14, 2019 post in Dr. Smith's ECG Blog: A subject well worth periodic review — is the concept of Terminal QRS Distortion ( T-QRS-D ).
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. What do you think?
The post 6 Cardiology Board Review Questions That Will Help You Pass the Boards appeared first on BoardVitals Blog. If you’d like more sample questions then follow this link to begin a free trial today.
Many huge thanks to the entire EM Cases team, Advisory Board, SREMI, the amazing guest experts and you, the listeners of the podcasts, readers of the blogs, viewers of the videos and participants in the course, for making 2017 another successful year for EM Cases! And here they are.
Heart Failure and Cardiomyopathy 19% Valvular Disease 15% Pericardial Disease 3% Congenital Heart Disease 3% Vascular Diseases 5% Systemic Hypertension and Hypotension 8.5% The post 5 Free Cardiology MOC Practice Questions appeared first on BoardVitals Blog. Every question comes with detailed explanations and rationales.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chest pain and diaphoresis. His ECG is shown: What do you think? Given the R-R interval = 1160 msecs. for the first 3 beats in this tracing ).
Case An 82 year old man with a history of hypertension presented to the ED with chest pain at 1211. Regular readers of Dr. Smith's ECG Blog are well familiar with what is perhaps my favorite Stephen Smith Adage = "You diagnose acute pericarditis at your peril!" STAT Echo and minimal troponin elevation then confirmed the diagnosis.
Never chest pain but had to treat as hypertensive emergency. In fact, severe hypertension by itself can lead to greatly increased oxygen demand and type 2 acute MI, sometimes with ST Elevation. In fact, severe hypertension by itself can lead to greatly increased oxygen demand and type 2 acute MI, sometimes with ST Elevation.
Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. Smith again: Whenever someone sends me an ECG for determination of OMI or Not OMI, I say: "Any patient with OMI can have an ECG that does not show OMI.
LBBB also has discordant STE in V1-V3 and STD in V5, 6 -- I will not be giving examples of this, as they are readily available all over the blog. A man in his sixties with chest pain, tachypnea, and hypertension Case 20. As always, LAD OMI need not meet STEMI criteria and usually does NOT! Chest Pain and RBBB.
In 2025, the demand for telehealth capabilities will only continue to grow, especially in managing chronic conditions like hypertension and heart disease. Telehealth Capabilities Telehealth has become an essential tool in modern cardiology, particularly for remote monitoring and consultations.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. His wife contacted the ambulance service after the patient experienced an episode of loss of consciousness. The syncope lasted about 2-3 minutes according to his wife.
Q waves in association with RBBB are usually not seen in anterior leads unless there is pulmonary hypertension or anterior infarction. I've copied KEY points from My Comment in the August 6, 2022 post in Dr. Smith's ECG Blog — regarding the answer to this question. Figure-1: The initial ECG in today's case.
Emre is a new Editor of the Blog. A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chest pain. You can find many examples on this blog attesting that. Written by Emre Aslanger.
Heart Failure and Cardiomyopathy 19% Valvular Disease 15% Pericardial Disease 3% Congenital Heart Disease 3% Vascular Diseases 5% Systemic Hypertension and Hypotension 8.5% The post FAQs about the Cardiology Recertification Exam appeared first on BoardVitals Blog. Sign up for a free trial today!
Steffen writes this case: "A few weeks ago I was able to recognize a STEMI because of what I had seen on your blog." "I He had no further risk factors for atherosclerosis besides hypertension. But when I took a look at the 12 lead-ECG I got a big smile on my face, because I remembered the ECG from your blog."
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chest pain. Chest Pain – Benign Early Repol or OMI?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content