This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
And as per ECG Blog #350 — this could represent Wellens ' Syndrome IF this chest lead T wave inversion was new and occurred in a patient who initially had a normal ECG, and then had an episode of transient CP that had resolved at the time this ECG with chest lead T wave inversion was recorded. PEARL # 3: An Often Forgotten Clinical NOTE.
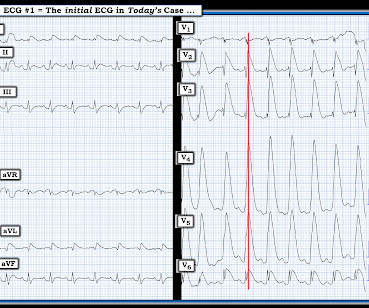
MY Impression of ECG #1: As emphasized often in this ECG Blog ( See today's ADDENDUM below ) — statistical odds that a regular WCT rhythm without clear sign of sinus P waves will turn out to be VT begin at 80% likelihood. See ECG Blog #287 — if interested in more on ECG recognition of AFlutter ). How Would You Treat this Patient?
For full discussion of this case — See ECG Blog #292 — == The 2 ECGs shown in Figure-1 were obtained from a man in his 30s — who presented to the ED ( E mergency D epartment ) with chest pain that began several hours earlier. Related ECG Blog Posts to Today’s Case: ECG Blog #205 — Reviews my Systematic Approach to 12-lead ECG Interpretation.
I i llustrate the ECG finding of T-QRS-D below in Figure-3 , which I've excerpted from My Comment in the November 14, 2019 post in Dr. Smith's ECG Blog. Today's case is also noteworthy in that T-QRS-D is seen in association with RBBB — which has only been described on rare occasions ( See the March 28, 2021 post i n Dr. Smith's ECG Blog ).
The "good news" — is that after an extended hospitalization, the patient was finally discharged home, and doing well. = As discussed in ECG Blog #364 and ECG Blog #265 — We are looking at " Shark Fin " ST elevation! ECG Blog #265 and ECG Blog #364 — Review cases of Shark-Fin ST Elevation.
For full discussion of this case — See ECG Blog #392 — == The ECG in Figure-1 was obtained from a man in his 60s — who described the sudden onset of "chest tightness" that began 20 minutes earlier, but who now ( at the time this ECG was recorded ) — was no longer having symptoms. ECG Blog #387 — Dynamic change in 2 minutes.
For more regarding ECG criteria for LVH — See the ADDENDUM below and/or ECG Blog #73 and ECG Blog #245. A bout H CM ( Different Forms of this Entity ): I've excerpted what appears below from My Comment in the December 26, 2023 post in Dr. Smith's ECG Blog. ECG Blog #245 — Reviews the ECG diagnosis of LVH.
As discussed in detail in ECG Blog #228 — this seemingly qualifies as a “ Silent ” MI ( Approximately half of those MIs not accompanied by CP — have some other associated symptom such as syncope, which substitutes as a “chest pain equivalent” ). ECG Blog #218 — Reviews HOW to define a T wave as being H yperacute ? What is T-QRS-D?
As discussed in many posts in this ECG Blog — despite not satisfying the millimeter-based definition of a STEMI — in this patient with new chest pain, the ECG findings in Figure-1 merit prompt cath lab activation without any need to wait for serum troponin to return elevated ( See ECG Blog #193 — regarding the new "OMI" paradigm ).
The ECG in Figure-1 was obtained from an 18-year old woman — who moments before been resuscitated from out-of-hospital cardiac arrest. An ICD ( I mplantable C ardiac D efibrillator ) was inserted — and the patient was discharged from the hospital. ECG Blog #185 — Reviews the P s, Q s, 3 R Approach to Rhythm Interpretation.
As reviewed in ECG Blog #350 — t he clinical significance of Wellens' Syndrome — is that its recognition tells you that the patient has a high-grade LAD narrowing with presumably "hot" thrombus h avin g high propensity to propagate and/or totally occlude the LAD at any point in time ( including immediately ). What is W ellens’ S yndrome ?
My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. Given this patient's older age — if nothing "fixable" is found, she most likely has SSS ( S ick S inus S yndrome ) and will need a pacemaker ( See ECG Blog #342 for more on SSS ).
For additional examples of this phenomenon whereby automatic truncation of an EMS ECG may mistakenly result in LVH serving to mimi c ischemia — Check out My Comment at the bottom of the page of the following posts in Dr. Smith's ECG Blog — the November 29, 2023 post — June 20, 2020 — March 31, 2019 — March 29, 2019 — and t he December 27, 2018 post.
The patient arrested outside the hospital. Does the patient's age infuence your interpretation? Figure-1: The initial ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ). Unfortunately — the cardiologist at that center did not recognize the abnormal ECG findings. He could not be resuscitated.
== P lease N OTE : After today — No new ECG Blog posts for 2- to -3 weeks. — I will also not be prompt in replying to emails. == All material on this ECG Blog site remains open! IF you scroll down a little on the right-hand column of this blog — You'll see a lot of icons. Figure-1: The initial ECG in today's case.
Although this " Imbalance " of precordial T waves is not see n very often — in the “right” clinical setting, it has been associated with recent OMI ( O cclusion-based MI ) , most often from a LCx culprit artery ( See Manno et al: JACC 1:1213, 1983 — and the July 17, 2013 post by Salim Rezaie in ALiEM — and ECG Blog #350 ).
The terminology favored to describe these ECG findings is diffuse subendocardial ischemia ( See ECG Blog #271 — for more on diffuse subendocardial ischemia ). The reason for this is simple — Most such patients die quickly , usually before they reach the hospital. Smith’s 8/9/2019 post in his ECG Blog.
By the P s, Q s, 3 R Approach ( See ECG Blog #185 ): Regarding R egularity — the rhythm is irregularly irregular. R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. . = ECG Blog #185 — Review of the P s, Q s, 3 R Approach for systematic rhythm interpretation.
The 12-lead ECG and long lead II rhythm strip shown in Figure-1 — was obtained from a previously healthy, elderly woman who collapsed in the hospital parking lot. These are reviewed in ECG Blog #343. I reviewed the concept of Echo beats in ECG Blog #239.
Hospital evaluation for this patient was negative for an acute coronary syndrome ( ie, CT coronary angiogram was normal — troponin was not elevated — and Echo was negative, with no sign of pericardial effusion ). See ECG Blog #215 — for more on the Cabrera format. = ECG Blog #114 — Reviews another case using the Cabrera format.
News & World Hospital Report rankings , we remind you this is only one of many tools you can use to have a conversation with your care team and should not be used as the sole factor when making decisions about your care. How do hospital rankings fit in? News & World Report ranks and rates hospitals. The post U.S.
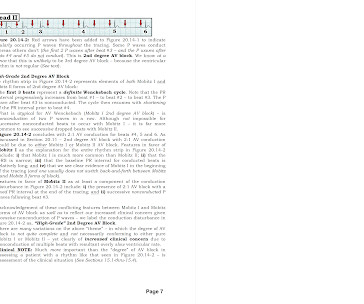
Assessing the Rhythm: I favor use of the P s , Q s , 3 R Approach for assessing the cardiac rhythm ( See ECG Blog #185 ). As emphasized in ECG Blog #326 ( and as I review in the ADDENDUM below ) — Mobitz I, 2nd-Degree AV Block ( ie, AV Wenckebach ) — is by far (!) ECG Blog #236 — Reviews the 3 Types of 2nd-Degree AV Block.
Seeing two brothers have HLHS is extremely rare and even more rare is how differently the condition presented in each child, says Childrens Hospital Colorado cardiothoracic surgeon Max Mitchell, MD, who performed the procedures on Zane and advised on Zekes care. We dont put limitations on them unless its for their safety, says Kayla.
Variations of this “theme” were seen on telemetry over the several days that this boy was in the hospital. MY Approach to the Rhythm in Figure-1: As always — I favor a systematic approach to rhythm interpretation — with use of the P s, Q s, 3 R Memory Aid ( See ECG Blog #185 for more on the Ps, Qs, 3Rs ).
With only one CT scanner in the hospital to service outpatients and the emergency room, Bonner General saw an urgent need for expansion in order to better serve its patients. Since 2014, Bonner General Health in Sand Point, Idaho, has experienced a staggering 73% increase in the number of CT scans they perform annually.
An ECG was recorded immediately at triage and, at this hospital, the Queen of Hearts is routinely used to determine cath lab activation. For more on ECG findings in pulmonary disease — Check out My Comment in the May 31, 2024 post in Dr. Smith's ECG Blog ). This patient had the onset of chest pain 24 hours before arrival to the ED.
He has been following the blog for 4 years. He has now implemented the Queen of Hearts in his hospital. This case was sent by Dr. Jean-christophe Reiters, an interventionalist in Belgium. He wanted to share one of the first cases. A 55 year old with no previous cardiac history presented with 3 hours of chest pain.
Each section includes: A brief check list of the OMI ECG criteria Several ECG examples curated from Dr. Smith's ECG Blog The specificity of each criteria with links to relevant literature ? Smith and Meyers ( that are well known to readers of this Blog ). I’ve accessed this hand OMI Pocket Guide on both my ipad and iphone.
Rural hospitals across the United States are currently grappling with a severe and precarious financial situation. Over the past decade, more than 100 rural hospitals have shut their doors , leaving vulnerable communities without vital healthcare access.
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. The rest of the patient’s hospital stay was uneventful and he was eventually discharged. Regular readers of this ECG Blog will be well familiar with many of these points. An ECG was finally done at 9:17am on the 2nd hospital day.
He was intubated in the field and sedated upon arrival at the hospital. At his family's request, he was transferred to a hospital closer to his home to continue care. The electrophysiologist is a reader of Dr. Smith's ECG Blog. When EMS arrived the patient was in ventricular fibrillation. He was admitted to cardiology.
News & World Hospital Report rankings , we remind you this is only one of many tools you can use to have a conversation with your care team and should not be used as the sole factor when making decisions about your care. How do hospital rankings fit in? News & World Report ranks and rates hospitals. The post U.S.
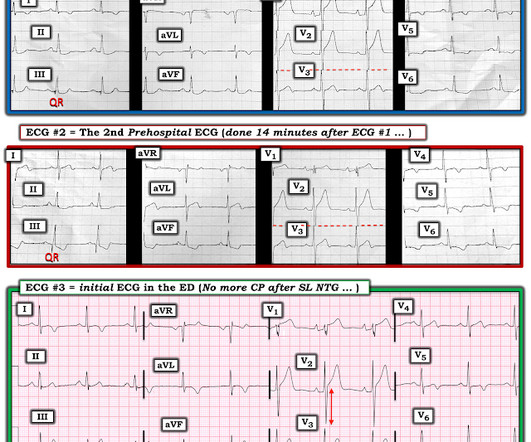
Written by Pendell Meyers I received this prehospital ECG (we receive prehospital ECGs by telemetry from EMS in a large area around our hospital) and was told that there was a patient in her 50s with chest pain who was headed to an outside hospital (which happens to be a catheterization center). Here is the ECG: What do you think?
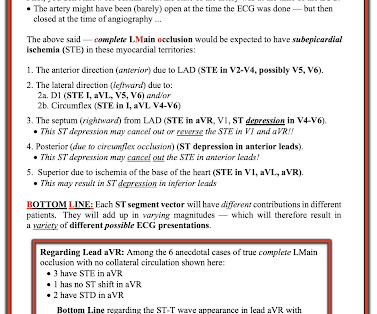
The patient was extubated on Day-3 of the hospital stay. The patient improved, and on Day-11 of the hospital stay — he was off inotropes and on a small dose of a ß-blocker. As we've often emphasized on Dr. Smith's ECG Blog — it is rare in practice to see LMCA occlusion, because most such patients die before reaching the hospital.
Once again, Cassling is teaming up with Bellevue University for a series of webinars that offer current and aspiring leaders with the top-of-license skills they need to make a difference for their teams, their hospitals, and their patients.
She presented to an outside hospital after several days of malaise and feeling unwell. Another possible cause of pseudonormalization of T waves mentioned many times on this blog is the pseudonormalization caused by re-occlusion of an infarct related reperfused coronary artery. At the time of admission, her vital signs were normal.
For clarity in Figure-1 — I've reproduced today's ECG — obtained following successful resuscitation of out-of-hospital cardiac arrest. As we have often emphasized on Dr. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! Figure-1: The initial ECG in today's case. —
In this blog, we’ll explore why fellowship programs are invaluable, when you should consider them in your career journey, and the transformative impact they can have on your professional trajectory. Expanded Career Options Fellows often transition into prestigious roles in hospitals, private practices, or academic institutions.
Complete Heart Block with Altered Mental Status Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the third installment of a blog series showing how transcutaneous pacing (TCP) can be difficult and how you can improve your skills. BVM was continued via NPA and the patient transported to the closest hospital.
In fact, most do not make it to the hospital alive, which explains why only a tiny percent of OMI are due to full LM occlusion. Today's patient did make it to the hospital — but was in cardiogenic shock, and despite valiant attempt at treatment, succumbed soon after. Moreover, left main occlusion often presents near death.
This blog is full of cases in which OMI that did not meet STEMI millimeter criteria were dismissed. Series of Prehospital ECGs Showing Reperfusion == MY Comment by K EN G RAUER, MD ( 9/21/2020 ): == I wish those cardiologists who continue to strictly adhere to STEMI millimeter criteria would begin reading Dr. Smith’s ECG Blog.
As is often emphasized on Dr. Smith's ECG Blog — the evolution of an acute OMI is not necessarily static — but may be "dynamic". For examples of this phenomenon — See My Comment in the February 14, 2018 — July 21, 2020 — and December 22, 2022 posts in Dr. Smith's ECG Blog ).
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. So the patient was admitted to the hospital with no plan for an angiogram. Edited by Smith He also sent me this great case.
Time is muscle” was the impetus for the new $6 million cardiovascular suite at Methodist Jennie Edmundson Hospital in Council Bluffs, Iowa. The longer you take to stabilize the heart, the higher the risk of long-term damage to the patient’s heart.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content