This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
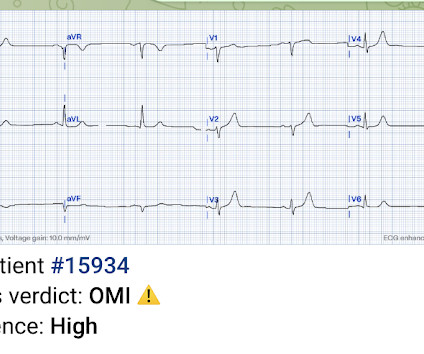
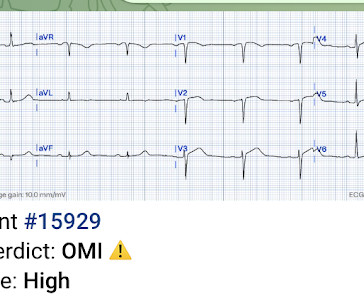
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
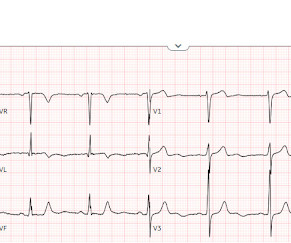
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. What is the gold standard for ECG interpretation: patient outcome!!!
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach.
Dr. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al.
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. Greater severity of chest pain is presumed to be associated with a stronger likelihood of a true positive STEMI diagnosis. years old ± 13.7
This is obviously unreliable data, as Dr. Smith’s Blog has published 51 cases of OMI with ECGs labeled ‘normal’ , 35 of which were identified by the Queen of Hearts – with 10 examples here. Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.
Safety of Computer Interpretation of Normal Triage Electrocardiograms. The cath lab was activated, as it should be with transient STEMI. See this case of transient STEMI: Spontaneous Reperfusion and Re-occlusion - My Bad Thinking Contributes to a Death. It is not yet available, but this is your way to get on the list.
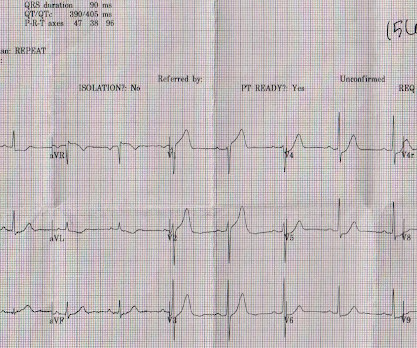
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." We have shown many examples of this on this blog.
You can see how V1, V2, aVR, and V4R would have ST elevation in either a right ventricular STEMI or with a septal STEMI, and how lateral leads, and even posterior leads, would have reciprocal ST depression. of patients with anterior STEMI, ST elevation of greater than or equal to 3.0 STE in V4R is confirmatory evidence.
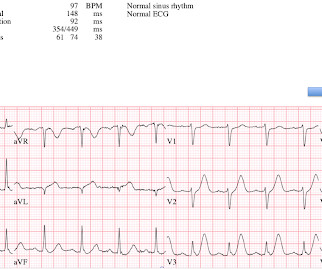
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Smith , d and Muzaffer Değertekin a DIFOCCULT: DIagnostic accuracy oF electrocardiogram for acute coronary OCClUsion resuLTing in myocardial infarction. His first electrocardiogram ( ECG) is given below: --Sinus bradycardia. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. Turk Kardiyol Dern Ars.
The patient with no prior cardiac history presented in the middle of the night with acute chest pain, and had this ECG recorded during active pain: I did not see any ischemia on this electrocardiogram. The patient has active chest pain, so if these are abnormally large T-waves This link shows 13 blog posts of Posterior Reperfusion T-waves.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. The LAD has reperfused early. This was recorded 2.5
can cause ST-segment elevation (STE) on electrocardiogram (ECG), the distinction between them may be hard and complicated. Furthermore, some ECGs may not meet the STEMI criteria but may still be diagnostic for acute coronary occlusion (ACO).
I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 mm of STE in II and III, or III and aVF, or V4 and V5, so some might say it fulfills STEMI criteria (remember, the interrater reliability of STEMI criteria is poor as shown in references below): McCabe et al. Carley et al. Emerg Med J.
The utility of the triage electrocardiogram for the detection of ST-segment elevation myocardial infarction. link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise!
An initial electrocardiogram (ECG) is provided below. As per Dr. Aslanger — a number of medical providers were initial confused by what initially appears as marked ST elevation with reciprocal ST depression, indicative of an acute STEMI. See My Comment at the bottom of the page in the May 19, 2020 post in Dr. Smith's Blog ).
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. So there was 3-vessel disease, but with an acute posterior STEMI. There is no ST elevation. See the list below.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch. A 12-lead electrocardiogram, lead V4R , and leads V7-9 were recorded on admission.
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He was worried for inferior MI and ordered another, which was recorded 15 minutes later: Now clearly and obviously diagnostic of inferior STEMI. Unknown algorithm Interpretation: Inferior ST elevation, with reciprocal ST depression in aVL.
This was marked as "Not a STEMI" by the physicians. It is not a STEMI, but it is diagnostic of an LAD OMI (Occlusion MI). That said — followers of Dr. Smith's ECG Blog have already seen numerous clinical cases that we have presented in which the PM Cardio AI Bot app. This was sent to me by a friend. What About the Initial ECG?
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI! Posterior STEMI occurs in approximately 15-20% of acute MI, but the vast majority of the time it is seen in conjunction with inferior (Infero-Posterior) or lateral (Postero-Lateral) STEMI (1).
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
This was just published in JAMA Internal Medicine: The de Winter Electrocardiogram Pattern Evolving From Hyperacute T Waves It reminded me that many believe, due to the assertions in the original de Winter's article, that de Winter's waves are stable. Interventionalist at the Receiving Hospital: "No STEMI, no cath. They are too narrow!
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Updates on the Electrocardiogram in Acute Coronary Syndromes.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 This T-wave inversion morphology is very specific for Wellens' waves. Computerized QTc = 417. Patel DJ, et al.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. So maybe she is better than I am. Heart Rhythm, 13(7): 1515-1520. [2]:
Below is the post -PCI electrocardiogram. For those in search of brief review of the Cabrera Format for ECG recording — Please check out My Comment at the bottom of the page in the October 26, 2020 post in Dr. Smith's ECG Blog. In the cath lab the patient was found to have a 100% occlusion of a small 1st marginal branch of the LCx.
STEMI was activated and the patient went to Cath on arrival. From Smith ECG Blog LCx occlusion There is aVR STE with broad STD, appreciable in both Leads II and V5. Readers interested in a more robust discussion of STD vectors, and their implications in OMI, are encouraged to read this phenomenal post at the Smith ECG Blog.
You will note that it is essentially an unremarkable electrocardiogram except for some PACS. At baseline, the patient has some expected, normal STE in lead V2, further demonstrating that the STD morphology in the presentation ECG above is "true" and diagnostic. This raised our concerns that the findings on his initial one were real.
Emergent cardiac outcomes in patients with normal electrocardiograms in the emergency department. These include about 60 occlusion MI (OMI) with clear ST segment elevation (none of which would be called “Normal” by the computer) and about 165 Non-STEMI. Am J Emerg Med. 2022 Jan;51:384-387. doi: 10.1016/j.ajem.2021.11.023. 2021.11.023.
3) STEMI criteria failed to identify this acute coronary occlusion, like many others. Learning Points: 1) As we have previously demonstrated, aVL was once again the key initial clue to diagnosing subtle RCA occlusion. 2) Contemporary troponins only start to rise 4-6 hours after the onset of acute coronary occlusion.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. Bicarb 20, Lactate 4.2,
cm diameter in the apex The presence of thrombus led the clinicians to state that this was a "late presentation STEMI." It does take some time for thrombus to form, but the EKG and the troponin profile show that this was NOT a late presentation STEMI. LV Thrombus , 1.5 0 0 1 95 544 MMRF 4 1 638 14.0 0 0 1 41 238 MMRF 1 1 278 14.0
Comment This paper has received some press recently: Safety of Computer Interpretation of Normal Triage Electrocardiograms The algorithm used was also the GE Marquette 12 SL. I don't know what her subsequent cardiac function was, but that is not the point of this post. But it could have been a disaster.
A Deep Neural Network learning algorithm outperforms a conventional algorithm for emergency department electrocardiogram interpretation. But lead V2 has a worrisome amount of ST elevation, and in a chest pain patient, I would be worried about STEMI. I do research on Cardiologs' algorithm: Smith SW et al. What an honor.
PCI mid LCx So this is an OMI (Occlusion Myocardial Infarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. This figure comes from the Diamond T study (all type 1 MI were NSTEMI, not STEMI): Notice that the 6 hour value (far right) is very low for type 2 MI. Angiogram: LM 30% ostial.
They recorded a prehospital ECG and diagnosed STEMI and activated the cath lab prehospital. The stress electrocardiogram is non-diagnostic. male with a history of HTN and ETOH developed squeezing epigastric abdominal pain with associated vomiting and diaphoresis, followed by a syncopal episode which lasted about 10 seconds.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content