This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
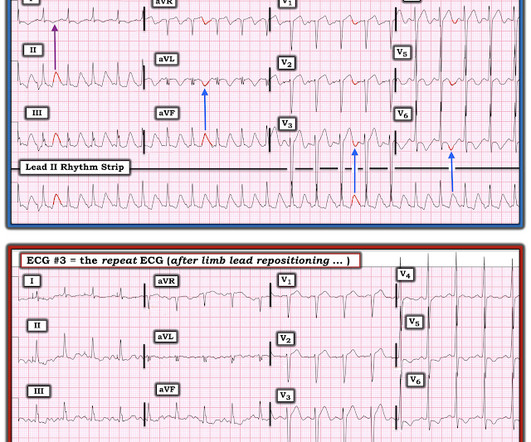
The patient with no prior cardiac history presented in the middle of the night with acute chest pain, and had this ECG recorded during active pain: I did not see any ischemia on this electrocardiogram. It does not look entirely normal, since there are some nonspecific STT abnormalities, such as flattening of the T waves in aVL.
Dr. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. Hence the first ECG was labeled 'anterior ischemia' based on ST depression, rather than identifying this as reciprocal from posterior OMI. But are there any other signs of Occlusion MI? Meyers et al.
5] Back to the case The patient had serial ECGs over the next hour with no significant change: The first troponin came back at 1,400 ng/L (normal <26 in males and <16 in females), confirming MI – and the patient’s refractory ischemia indicated this was an Occlusion MI. Clin Cardiol 2022 4. Herman, Meyers, Smith et al.
An initial electrocardiogram (ECG) is provided below. Learning Point: Concordant ST segment elevation can arise from profound ischemia triggered by ventricular tachycardia (VT), or it may represent an exaggerated basal ST change accompanying tachycardia. The patient was promptly admitted to the hospital for further evaluation.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] There is evolution from Wellens Pattern A to Pattern B, now inclusive of V6.
Chest Pain Severity Rating Is a Poor Predictive Tool in the Diagnosis of ST-Segment Elevation Myocardial Infarction [link] Abstract Current ST-segment elevation myocardial infarction (STEMI) guidelines require persistent electrocardiogram ST-segment elevation, cardiac enzyme changes, and symptoms of myocardial ischemia.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
Precordial ST depression may be subendocardial ischemia or posterior STEMI. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. Whether it is subendocardial ischemia or posterior STEMI, if you cannot get it to resolve, you must activate the cath lab. There is no ST elevation.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
In other words, the inferior ST segments in the first ECG show more straightening which is more concerning for ischemia. Below is the post -PCI electrocardiogram. For more on this mirror-image opposite ST-T wave relation in leads III vs aVL — See My Comment in the March 8, 2019 and August 9, 2018 posts in Dr. Smith's ECG Blog ).
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." When the ischemia is resolved, the wall motion may completely recover, or there may be persistent stunning.
Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. But the real question at hand is: Are these precordial ST-depressions a result of subendocardial ischemia?
This was just published in JAMA Internal Medicine: The de Winter Electrocardiogram Pattern Evolving From Hyperacute T Waves It reminded me that many believe, due to the assertions in the original de Winter's article, that de Winter's waves are stable.
She requires maximal medical management per all current guidelines (including heparin and P2Y12 inhibitor per cardiology), as well as consideration for emergent cath in the case of persistent ischemia. So what will you do for this patient? They found an acute, total, thrombotic occlusion of the proximal LAD. They opened it. Patel et al.,
The stress electrocardiogram is non-diagnostic. This ST-T wave appearance in the lateral chest leads of ECG #2 is consistent with L V “ S train” vs ischemia. No wall motion abnormality at rest. No wall motion abnormality with stress. Next day, a stress echo was done: The exercise stress echocardiogram is normal.
Background: The value of the 12-lead ECG in the diagnosis of non-ST-elevation myocardial infarction (NSTEMI) is limited due to insufficient sensitivity and specificity of standard markers of ischemia and because ECG confounders may prevent their application. Journal of Electrocardiology 3(2):161-167; 1970.
EKG shown here: LAFB with no clear signs of OMI or ischemia. Interestingly, this patient was seen in the ED for hypertension and headache 3 days earlier. No labs were performed. EKG and CT head were performed. Imaging was negative and he was discharged home.
The patient continued to have ischemia after PCI, and in fact had an episode of polymorphic VT shortly after while in the ICU. Clinical value of 12-lead electrocardiogram after successful reperfusion therapy for acute myocardial infarction. This was recorded 2.5 Reexamining the "gold standard" for myocardial reperfusion treatment.
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. You will note that it is essentially an unremarkable electrocardiogram except for some PACS. The morphology in V2 is also concerning and it appears that the ST segment is being pushed down, as in ST depression.
Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. Figure-1: ECG criteria for diagnosis of a Brugada-1 or Brugada-2 pattern ( See text ). == N OTE : There are numerous additional cases regarding Brugada pattern ECGs by Dr. Smith on this blog ( Simply search for Brugada Syndrome! ).
More likely, the patient had crescendo angina, with REVERSIBLE ischemia for 48 hours that only became potentially irreversible (STEMI) at that point in time. During the 48 hours of angina, such reversible ischemia often leads to myocardial stunning with akinesis of the myocardial wall that puts it at risk for thrombus.
Electromechanical association: a subtle electrocardiogram artifact. Arterial pulse tapping artifact [link] This online article references the article below by Emre Aslanger, a great guy who occasionally corresponds with me about ECGs. Aslanger E, Yalin K. Journal of Electrocardiology. 2012;45(1):15-17. doi:10.1016/j.jelectrocard.2010.12.162.
A Deep Neural Network learning algorithm outperforms a conventional algorithm for emergency department electrocardiogram interpretation. This ECG comes from Pierre Taboulet ( [link] /)( [link] ) an ECG whiz who codes a lot of ECGs for Cardiologs' Artificial Intelligence Deep Neural Network algorithm ( [link] ). What an honor.
Across both selected patient populations, the positive predictive value was highest in patients with chest pain, with ischaemia on the electrocardiogram, and with a history of ischaemic heart disease. to 62.2%) in the UK and 4.2% (68/1631) and 16.4% (13.0% to 20.3%) in the US.
Abnormal Electrocardiogram (ECG): Defined (San Fran syncope rule) as any new changes when compared to the last ECG or presence of non-sinus rhythm. Evidence of acute ischemia (may be subtle) vii. Electrocardiogram-based risk stratification was useful in guiding the use of specialized cardiovascular tests. __ 9) François P.
I suspect most blog readers did not struggle with this one. Artificial intelligence (AI) algorithms show promise to improve electrocardiogram (ECG) interpretation. Toward this end we've conveniently added a LINK for "LVH Criteria" in the Menu at the top of every page in Dr. Smith's ECG Blog. Figure-1: I've labeled today's ECG.
The de Winter electrocardiogram pattern is an infrequent presentation, reported to occur in 2% to 3.4% In this situation, even after the ischemia is relieved and myocardial blood flow is restored myocardial contractile function remains impaired for a variable period of time (usually days to a few weeks). References: Kloner, R.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content