This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This blog explores how genetics influence heart health and whether mitigating these inherited risks is possible. Specific genetic variants, such as those affecting cholesterol metabolism, can increase the likelihood of plaque buildup in the arteries. Heart imaging, such as echocardiograms or CT scans.
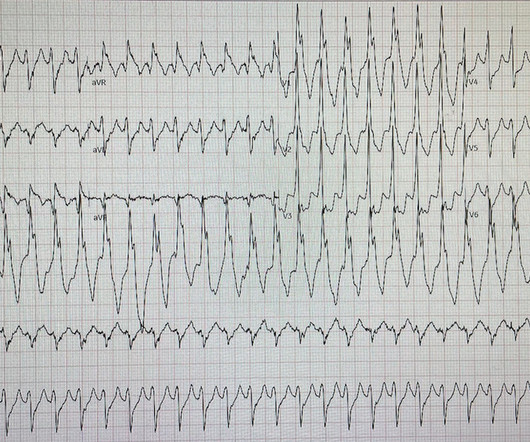
I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. Readers of the Smith ECG Blog will probably recognize this a very subtle inferior OMI. Corresponding echocardiogram demonstrated LV systolic dysfunction with an EF 30%. Examples provided below.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. It is not rare.
Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function. His ECG at the accepting facility is shown below: Accepting facility ECG The team reviewed his angiography films with an interventionalist and thought they were suspicious for plaque rupture in LAD, but they were not confident.
Mild Plaque no angiographically significant obstructive coronary artery disease. I looks as if there has been reperfusion. PM Cardio AI Bot: Not OMI with high confidence Angiogram: Speckle Tracking of Acute Pulm Edema.MOV from Stephen Smith on Vimeo.
Because: 1) He has been reading this blog for a long time. The scan did not find PE, but showed evidence of coronary plaque: There are areas of dense white in the LAD (red and blue circles) and in the first diagonal (green circle). An echocardiogram showed an EF of 20-25%. 2) He is curious This is how Pendell got started.
She underwent exercise echocardiogram in mid October where she exercised for nearly 7 minutes on the standard Bruce protocol and had typical anginal pain and shortness of breath. Baseline echocardiogram showed moderate LV systolic dysfunction with no wall motion abnormalities. Conduction defects can also be intermittent.
The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. Bedside echocardiogram showed hypokinesis of the mid to distal anterior wall and apex. Smith comment : a very high proportion of MINOCA are ruptured plaque with lysed thrombus.
Here is the cath report: Echocardiogram: There is severe hypokinesis of entire LV apex and apical segment of all the walls. To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! ng/mL by 4th generation and older assays.)
ECG 2 Especially in the context of the first ECG, readers of this blog will readily appreciate the ST elevations and hyperacute T waves in II, III, aVF, V6, and to a lesser extent V5. As an aside, the LCx OMI is a type 2 event, since it is due to supply-demand mismatch from thrombus, and not due to atherosclerotic plaque rupture or erosion).
With this test, an echocardiogram is done at rest to study the pumping ability of the heart. With time, fat and cholesterol can get trapped in the areas of wear and tear and cause plaque formation. The plaques can damage us in 2 ways.
Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. The initial troponin I was elevated at 0.75
See this case: what do you think the echocardiogram shows in this case? We’ve presented many variations on this theme on Dr. Smith’s Blog — with today’s case being distinguished by its discovery on abdominal exam ! Widespread ST-depression with reciprocal aVR ST-elevation can be cause by: Heart rate related: tachyarrhythmia (e.g.,
So today i wanted to talk to you about what each heart test tells us about these different aspects of heart disease Tests that tell you about the heart as a pump The most commonly used test to assess the heart as a pump is an echocardiogram. Overall though a normal cardiac MRI is even more reassuring than a normal echocardiogram.
She was treated medically for NonSTEMI, pending next day cath, which showed ulcerated plaque and a 60% thrombotic stenosis in the LAD distal to the first diagonal. A formal contrast echo was done at this point : Normal estimated left ventricular ejection fraction, 65%. Regional wall motion abnormality-distal septum and apex. It was stented.
Angiogram: Severe coronary artery calcification Moderate to severe distal small vessel disease mainly seen in RPL1, 2 Otherwise, Mild plaque, no angiographically significant obstructive coronary artery disease. Echocardiogram: Estimated left ventricular ejection fraction, lower limits of normal; 45-50%.
These are reperfusion T-waves (the same thing as Wellens' waves) Echocardiogram Regional wall motion abnormality-distal septum and apex. Regional wall motion abnormality-distal inferior wall. ECG recorded at time 38 hours: A further evolutionary stage of T-wave inversion.
In this study of consecutive patients with LBBB who were hospitalized and had an echocardiogram, a QRS duration less than 170 ms (n = 262), vs. greater than 170 ms (n = 38), was associated with a significantly better ejection fraction (36% vs. 24%). So indeed the QRS is approximately 200 ms. Comment: What is the normal QRS duration in LBBB?
The intricacies of the different classes of antiarrhythmics and their mechanism of action extend beyond the scope of this blog. There were no plaques or stenoses. I list below links to other cases of idiopathic VT from Dr Smith's ECG blog. It is reasonable to perform an echocardiogram to evaluate LV function.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content