This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
For more regarding ECG criteria for LVH — See the ADDENDUM below and/or ECG Blog #73 and ECG Blog #245. A bout H CM ( Different Forms of this Entity ): I've excerpted what appears below from My Comment in the December 26, 2023 post in Dr. Smith's ECG Blog. ECG Blog #245 — Reviews the ECG diagnosis of LVH.
EKG with paced complexes shown below shows much narrower QRS complex and echocardiogram showed improved LV systolic function primarily due to improvement in LV dyssynchrony. (J For more on Torsades de Pointes vs PMVT See My Comment in the October 18, 2023 post and the September 2, 2024 post in Dr. Smith's ECG Blog ).
This case was posted on the [link] ultrasound site, of which this ECG blog is a part. However, only the first ECG was shown, and it was recorded before the patient became ill. I refer you to the video case presentation by one of my colleagues, Dr. Rob Reardon (who has, by the way, a fantastic collection of ED ultrasound cases).
What do you think the echocardiogram shows? I have posted previous such cases, but in searching my own blog, I could not find them. Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardial infarction, likely proximal LAD or Left main." NTG drip started. Pain better still.
Date Nov 7, 2024 Image Blog Giving Credit Matters. Image Blog Managing Relationships with Patients Early career cardiothoracic surgeons have many important relationships that need to be managed and developed. Here's How to Do It. The coronary vessel anastomosis session and the CPB/echo room were outstanding.” “The
This blog explores how genetics influence heart health and whether mitigating these inherited risks is possible. Heart imaging, such as echocardiograms or CT scans. Understanding the Genetic Connection to Heart Disease Your genetic makeup plays a vital role in shaping your heart health.
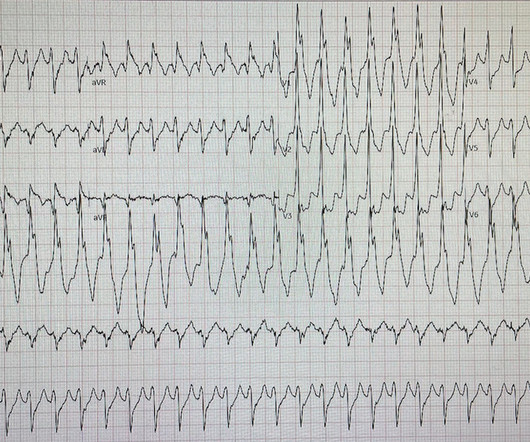
Readers of the Smith ECG Blog will probably recognize this a very subtle inferior OMI. Corresponding echocardiogram demonstrated LV systolic dysfunction with an EF 30%. The VT vs SVT with Aberrancy debate is beyond the scope of this particular blog post. Here is the ECG after 200J. Examples provided below.
Smith comment: Go here for a comprehensive blog post on syncope and link to the most detailed version of the Canadian Syncope Rule: Emergency Department Syncope Workup. See these blog posts. The echocardiogram showed a normal EF without any abnormalities. Although it is somewhat of a misnomer, it portends high grade AV block.
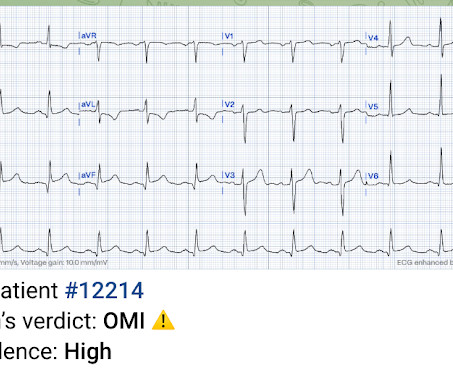
A 49 year old woman with h/o COPD only presented with sudden dyspnea. She had acute pulmonary edema on exam. Prehospital Conventional algorithm interpretation: ANTERIOR INFARCT, STEMI Transformed ECG by PM Cardio: PM Cardio AI Bot interpretation: OMI with High Confidence What do you think?
It is a known OMI mimic that we have shown on the blog many times. The emergent echocardiogram showed normal EF, no WMA, and normal valve function. This situation has been named "Emery phenomenon." In other words, the inferior "ST elevation" is due to the abnormal rhythm, and does not signify OMI or STEMI in any way.
See this post: What do you think the echocardiogram shows in this case? Previously placed stents in the LAD (multiple) and mid circumflex and patent Formal echocardiogram: Normal left ventricular size and wall thickness. Shortly thereafter , the troponin came back at 3,129 ng/L (very high).
Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function. The electrophysiologist is a reader of Dr. Smith's ECG Blog. The above said — it may prove insightful to take another look at the Wellens' Syndrome case instantly recognized by Dr. Smith in the August 12, 2022 post in Dr. Smith’s ECG Blog.
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum.
This would have been fairly easy and much more expedient to diagnose with bedside echocardiogram. The constellation of dyspnea, tachycardia, and (relatively) low voltage on ECG should prompt immediate evaluation for pericardial effusion and tamponade.
Formal echocardiogram: Systolic function is at the lower limits of normal. We have shown many examples of this on this blog. To add to this complexity ( as per My Comment in the August 22, 2020 post in Dr. Smith's ECG Blog ) — the ST-T wave appearance in repolarization variants may be dynamic ! No further follow up is available.
Because: 1) He has been reading this blog for a long time. An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus. An echocardiogram showed an EF of 20-25%. This is another case sent by the undergraduate (who is applying to med school) who works as an EKG tech.
And then a slightly more remote past ECG Old inferior MI The patient's previous echocardiogram report was viewed: Decreased LV systolic performance, estimated left ventricular ejection fraction is 35%. Case continued The patient underwent an emergency formal echocardiogram and it was unchanged. Cath Lab activation was cancelled.
She underwent exercise echocardiogram in mid October where she exercised for nearly 7 minutes on the standard Bruce protocol and had typical anginal pain and shortness of breath. Baseline echocardiogram showed moderate LV systolic dysfunction with no wall motion abnormalities. There is inferoseptal hypokinesis.
So the artery had completely spontaneously reperfused prior to intervention; the duration of occlusion was perhaps 2 hours The troponin peaked at 60,000 ng/L (a very large infarction) Formal bubble contrast echocardiogram --The estimated left ventricular ejection fraction is 46%. Regional wall motion abnormality-inferior.
The post 6 Cardiology Board Review Questions That Will Help You Pass the Boards appeared first on BoardVitals Blog. Question banks are a favorite exam preparation resource for Cardiologists that want to practice in the format of the exam. If you’d like more sample questions then follow this link to begin a free trial today.
Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. A formal echocardiogram for patient 2 showed normal LV size, wall thickness, and global systolic function. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”.
A rapid echocardiogram was performed, revealing an ejection fraction of 20% with thinning of the anterior-apical walls. See My Comment at the bottom of the page in the May 19, 2020 post in Dr. Smith's Blog ). The initial troponin T level was measured at 30 ng/L.
Formal Echocardiogram: Normal left ventricular size and wall thickness. As I emphasized in My Comment at the bottom of the page in the October 10, 2022 post in Dr. Smith's ECG Blog — Interpretation of a post-resuscitation ECG can be extremely challenging. First — Some thoughts on the post -resuscitation ECG.
Echocardiogram was obtained and showed mild LVH without regional wall motion abnormality. For a list of lead reversal cases we've discussed in Dr. Smith's ECG Blog — GO TO the bottom of the page in My Comment from the January 6, 2024 post). Following PCI, the patient ruled out by troponins : troponin increased to 0.08 ng/mL and 0.10
His echocardiogram showed normal wall motion. From My Comment in the November 14, 2019 post in Dr. Smith's ECG Blog: A subject well worth periodic review — is the concept of Terminal QRS Distortion ( T-QRS-D ). The patient did well afterward without any recurrence of symptoms. There are no further EKGs or troponin measurements.
This is the world’s only AI platform built on the world’s largest database of echocardiograms linked to mortality. One of our partners, Echo IQ, recently sought FDA approval for their AI-based cardiology workflow, EchoSolv.
The area of insult was indeed large, but whether that area is all irreversibly infarcted or not would require MRI or a 6 week followup ("convalescent") echocardiogram, to see how much myocardium recovers (was only "stunned", not infarcted) Post PCI EKG: There is loss of anterior forces (Q-waves) which was not there before.
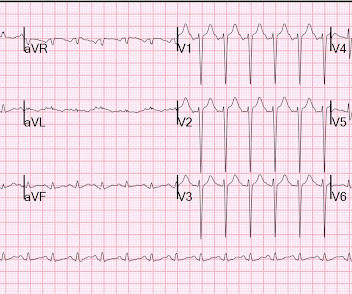
Nossen also pointed out that with voltage this high in the limb leads, you would typically expect some degree of inferior/inferolateral ST depression (the so-called "LVH strain" pattern), and in fact this patient did have severe LVH on subsequent echocardiogram (which Dr. Nossen did not know at the time). The troponin peaked at 25749 ng/L.
Echocardiogram showed severe RV dilation with McConnell’s sign and an elevated RVSP. Nicholson and Meyers provide numerous links at the end of their discussion to insightful related cases of acute PE that we've presented in Dr. Smith's ECG Blog. The patient was upgraded to the ICU for closer monitoring.
Hopefully a repeat echocardiogram will be performed outpatient. I've copied KEY points from My Comment in the August 6, 2022 post in Dr. Smith's ECG Blog — regarding the answer to this question. Systolic function normal by visual assessment only, unable to visualize well for further characterization. 2300: QRS now within normal limits.
We have shown that morphine is associated with worse outcomes (see learning points below) and have published many blog posts about it , such as this one: Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mass delusion (and Opiate pain relief). The case continues. The patient suffered a large infarct.
ECG 2 Especially in the context of the first ECG, readers of this blog will readily appreciate the ST elevations and hyperacute T waves in II, III, aVF, V6, and to a lesser extent V5. As discussed on this blog many times before, proportionality is key to the diagnosis of OMI by ECG. [link] I also texted the ECG to Dr. Smith.
Echocardiogram showed an anteroapical wall motion abnormality. This is highly suspicious for acute anterior STEMI. However, she was found to have a fatal pontine hemorrhage and had a maximum troponin I, at 12 hours after presentation, of 2.0
In this study of consecutive patients with LBBB who were hospitalized and had an echocardiogram, a QRS duration less than 170 ms (n = 262), vs. greater than 170 ms (n = 38), was associated with a significantly better ejection fraction (36% vs. 24%). Here is a similar case involving right bundle branch block.
Echocardiogram is indicated (Correct) C. Start aspirin and Plavix Correct answer: (B) (B) Echocardiogram is indicated. The post Hypertropic Cardiomyopathy: A Board Review Question Explained By Video appeared first on BoardVitals Blog. Which of the following is the best statement to describe further clinical management?
Here is the post PCI EKG: And a few hours after that: The post PCI echocardiogram showed: Normal estimated left ventricular ejection fraction, 57%. This is a large OMI that has Zero ST Elevation but can be diagnosed by ECG features other than ST Elevation!! Regional wall motion abnormality-mid to basal inferior wall.
A stat echocardiogram would have helped to make this diagnosis and facilitate timely reperfusion. Possibilities include: serial ECGs (which were done but still nondiagnostic), stat echocardiogram, or posterior ECG. Pain is similar, but associated with less SOB. Exam is unremarkable.
Echocardiogram: The estimated left ventricular ejection fraction is 34% Regional wall motion abnormality-lateral, akinetic. Selected LINKS for More on the Mirror Test: ECG Blog #246 — Reviews the concept of the "Mirror Test" with a clinical example. A massive acute OMI.
An echocardiogram confirmed aortic stenosis with a large pressure gradient. Now there is much less ST segment deviation, less elevation and less depression. The troponin returned positive, and the maximum troponin was 3.8 The next day, and angiogram showed normal coronary arteries. He awoke and did well.
These specialized functionalities encompass advanced ECG interpretation, seamless stress test reporting, and the integration of diverse imaging modalities, such as echocardiograms and MRIs. Cardiology-specific EHR software seamlessly integrates data from echocardiograms, MRIs, and other cardiac imaging sources.
The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. Bedside echocardiogram showed hypokinesis of the mid to distal anterior wall and apex. Initial hscTnI was 10 ng/L (ref. <14). There was no recommendation for repeat ECG.
The echocardiogram shows a preserved left ventricular ejection fraction (LVEF) of 55% with marked basal and mid inferolateral and basal anterolateral hypokinesia. As we often note in Dr. Smith's ECG Blog — there normally should be slight, upward sloping ST elevation in leads V2 and V3. Good angiographic result.
This blog explores the profound benefits of AI and machine learning, which are revolutionizing cardiology practices, enhancing efficiency, and ultimately improving patient care. These technologies are not just reshaping but also empowering how cardiology practices manage operations, deliver care, and enhance patient outcomes.
The diagnosis was a bit hard to find in the chart, and the echocardiogram did only stated "assymetric hypertrophy." For MORE on Some of the Concepts I Comment On: Re the ECG findings in HCM ( H ypertrophic C ardio M yopathy ) — See My Comment at the bottom of the page in the October 28, 2023 post in Dr. Smith's ECG Blog.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content