This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In this ECG Cases blog Dr. Jesse MacLaren guides us through 10 cases of patients who present with generalized weakness or acute neurologic symptoms and discusses how to look for ECG signs of dysrhythmias, electrolyte emergencies, acute coronary occlusion, and demand ischemia in patients with generalized weakness and in patients with neurologic symptoms, (..)
Because she has cardiomyopathy and ventricular dysrhythmias, the pacer included an Implanted Cardioverter-Defibrillator (ICD) Echo 6 days later after CRT: Normal estimated left ventricular ejection fraction. The septum is punctured with the active fixation screw of the lead - so essentially you bore the septum with the screw helix."
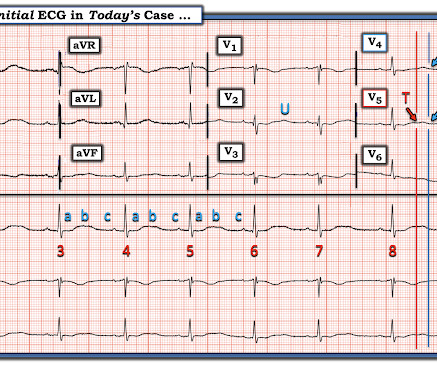
Especially when present in the setting of bradycardia and syncopal episodes, this is very worrisome for high risk of lethal dysrhythmias including polymorphic ventricular fibrillation (termed Torsades when in the setting of long QT). This ECG shows sinus bradycardia with massively long QT (or QU?) interval, at over 600 msec.
In that sense, the term dysrhythmia is preferable because it does literally translate as a disturbance in normal rhythm which is exactly what it is meant to describe. Any unsolicited disturbance of the rate or rhythm can be termed a dysrhythmia and result in the heart beating less efficiently but only for the duration of the dysrhythmia.
See these publications for more information Overall, management for cardiac contusion is mostly supportive unless surgical complications develop, involving appropriate treatment of dysrhythmias and hemodynamic instability. Figure-1: The initial ECG in today's case. What are the ECG Findings of Cardiac Contusion?
If you don't know what the dysrhythmia is, then try procainamide. Lessons from Today's CASE: I've reviewed "My Take" on ECG interpretation of the regular WCT rhythm on many occasions in Dr. Smith's ECG Blog ( See My Comment at the bottom of the page in the June 23, 2023 post , among many others ). What to do now?
Flecainide : This is a potentially dangerous Na channel blocker which can cause ventricular dysrhythmias including ventricular fibrillation. For more on AFlutter — Please check out My Comment in the November 12, 2019 post and the May 1, 2023 post in Dr. Smith's ECG Blog ). She is already anti-coagulated, so that is not an issue.
Relative contraindications to both include a known prolonged QT, especially if the dysrhythmia is believed to be caused by prolonged QT. Another benefit: Procainamide is very effective at terminating SVT. So if you are incorrect about your diagnosis, it might convert with procainamide anyway!
No patient with a QRS of less than 160 ms had ventricular dysrhythmias. Blockade of cardiac fast sodium channels (leads to wide QRS, R-wave in aVR, R' wave in V1, Brugada pattern ECG, ventricular dysrhythmias.) Articles on TCA More TCA ECGs from Dr. Smith's ECG Blog More on TCA overdose, with ECGs, from life in the fast lane.
The patient himself had never had syncope or dysrhythmias. He proceeded also with an implantable loop recorder to detect subclinical dysrhythmias, and this was negative. Without Brugada pattern on the baseline ECG, there is no Brugada syndrome. However, there is an uncertain history of sudden death as well as inducible Brugada pattern.
The patient was admitted to the cardiology service with a plan for EP study, however the cardiologist during that visit thought that the ECG showed only LBBB, and thought that the patient's dysrhythmia was atrial fibrillation with LBBB, instead of atrial fibrillation with WPW. So he was simply discharged without EP study.
Is it sinus or is it a supraventricular dysrhythmia? If rapid, that means that the depolarization is rapidly advancing and that it must be using conducting fibers (Purkinje fibers), and is therefore supraventricular.
There were no dysrhythmias on cardiac monitor during observation. This discussion comes from this previous post: Hyperthermia and ST Elevation Discussion Brugada Type 1 ECG changes are associated with sudden cardiac death (SCD) and the occurrence of ventricular dysrhythmias. He was found to be influenza positive. Is there fever again?
He has a great blog too: ECG Interpretation He is also well known on the Facebook EKG Club page , where you can learn tons about ECGs: Here is his response, with the first ECG labelled: Hello Steve & Avinash. It is commonly seen in the reperfusion setting. It appears to be benign in children as well (see references below). What is it?
A lot of people have contacted me and asked me as to how to safely stop Beta blockers and therefore I thought I would do a quick blog on this subject. There have also been reports of heart failure status worsening and blood pressure going up excessively. This is termed as ‘Acute beta blocker withdrawal syndrome’.
Blunt cardiac injury my result in : 1) Acute myocardial rupture with tamponade 2) Valve rupture (tricuspid, aortic, mitral) 3) Coronary thrombosis or dissection (and thus Acute MI) from direct coronary blunt injury 4) Dysrhythmias of all kinds. Localized bleeding from contusion could cause hemopericardium even without rupture.
But adenosine only lasts for seconds, and if the dysrhythmia recurs, then the adenosine is gone. Prevent the initiation of the dysrhythmia -- this can be done with a beta blocker by prenenting PACS 2. Smith: should we give adenosine again? Adenosine worked. It converted the rhythm. We need to do one or both of two things: 1.
The second explanation (AIVR), whether as a reperfusion dysrhythmia or not, seems most likely. A repeat ECG had sinus rhythm at a rate of 54 and normal conduction (no LBBB), and was completely normal with no ischemia. The slow sinus rate supports the notion that this could be rate-related BBB.
Likewise, in some cases of ischemia concealed by flutter waves, the ischemia can be seen despite the flutter waves, whereas in other cases the dysrhythmia must be terminated before the ischemia can be clearly distinguished. Even when flutter waves conceal true ST segment deviations, the cause and effect relationship may be unclear.
So the real QT is shorter, but the computer does not mention the U-wave, and the U-wave is as important as the T-wave in predicting cardiac dysrhythmias. There is a very prominent U-wave and some of what may appear to be a QT interval is a QU interval. This is an extremely dangerous ECG. The K returned at 1.9 This is extremely low for DKA.
Opinions vary widely on the K level at which a patient must be admitted on a monitor because of the risk of ventricular dysrhythmias. My rationale is that if the K is affecting the ECG, then it is affecting the electrical milieu and can result in serious dysrhythmias. Until some real data is available, my opinion is this: 1.
Could the dysrhythmias have been prevented? Severe hypokalemia in the setting of STEMI or dysrhythmias is life-threatening and needs very rapid treatment. mmol/L (n = 11), and Measurements and Results: All patients tolerated the infusions without evidence of hemodynamic compromise, ECG change, or new dysrhythmia requiring treatment.
He was admitted for monitoring, as his risk of a ventricular dysrhythmia as cause of the syncope is high ( very high due to HFrEF and ischemic cardiomyopathy ). ECG 3 hours later was unchanged He was not started on heparin as type II MI was favored over NonSTEMI as the etiology of his troponin elevation.
The limb lead abnormalities appear to be part of the Brugada pattern, as described in this article: Inferior and Lateral Electrocardiographic RepolarizationAbnormalities in Brugada Syndrome Discussion Brugada Type 1 ECG changes are associated with sudden cardiac death (SCD) and the occurrence of ventricular dysrhythmias.
Then there is loss of pulses with continued narrow complex on the monitor ("PEA arrest") Learning Points: Sudden witnessed Cardiac Arrest due to ACS is almost always due to dysrhythmia.
Meyers, Smith; Weingart wrote an extensive review on Idiopathic VT in the September 14, 2018 post of Dr. Smith’s ECG Blog. As a result — it’s worth briefly reviewing this entity of “ Idiopathic ” VT. My Comment at the bottom of this Sept. 14, 2018 post adds a series of PEARLS on “My Take” regarding this subject.
Atrial dysrhythmias, and atrial fi brillation in particular, are frequently misdiagnosed by computer algorithms and then by the physician who overreads them. M Y A NSWER: The issue of whether C omputerized E CG I nterpretations are “at fault” for an inaccurate ECG diagnosis has been addressed numerous times on this blog.
I also believe that we physicians and medics are eager to treat dysrhythmias, and we want to see them even when they are not there. Dilated pupils and hypertension are a strong clue to sympathetic overload, but don't forget anticholinergic syndromes, including tricyclics!
The heart is an electrical organ and occasionally the electrics can choose to malfunction and the patient may develop a heart rhythm disturbance or a dysrhythmia such as AF or SVT or VT. Cardiac CT is now widely available and to my mind the easiest way to know about the blood vessels of the heart. You can only diagnose it in retrospect.
Inferior MI results in scar tissue which is a likely source of a re-entrant ventricular dysrhythmia. Here is the post-cardioversion ECG: There is sinus with RBBB There are inferior Q-waves suggesting old inferior MI. This would be the likely source of the VT.
I could find very little literature on the treatment of severe life-threatening hypokalemia. There is particularly little on how to treat when the K is less than 2, and/or in the presence of acute MI.
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. (For those of you who are accustomed to the units of high sensitivity troponin (ng/L), this is equivalent to 20,956.00 Again, cath lab was not activated. What does this troponin level mean?
Smith comment: In a large randomized trial of dopamine vs. norepinephrine (11) for shock which was published after the above-mentioned recommendations, dopamine had more adverse events (especially severe dysrhythmias, and especially atrial fibrillation).
Here is one full text article on the topic from Clinical Cardiology 2008: Diagnostic Approach and Treatment Strategy in Tachycardia-induced Cardiomyopathy Atrial Tachycardia (AT): another SVT in the ED Rapid dysrhythmia from non-sinus focus above AV node. E CG # 2 in Figure-1 is from the October 16, 2019 post on Dr. Smith’s Blog.
Sinus tach is often misinterpreted as a dysrhythmia. They often have good ejection fraction and tolerate the dysrhythmia quite well. There is no evidence that this elderly patient has suffered from VT or other primary dysrhythmias in the past. See this case, for example: A Relatively Narrow Complex Tachycardia at a Rate of 180.
He was admitted for monitoring and had no dysrhythmias. Although this is not a common phenomenon You will see it on occasion ( See the June 30, 2023 post the November 27, 2023 post and the July 24, 2013 post in Dr. Smith's ECG Blog ). Amazingly, the Queen also recognizes it as "Not OMI". She is very good.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content