This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
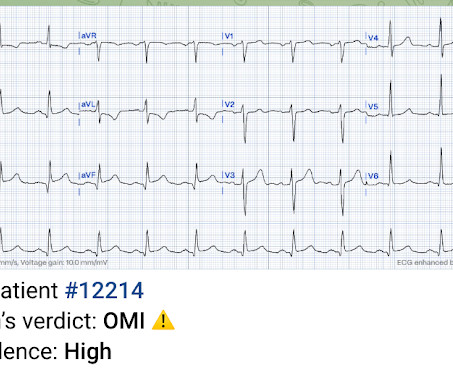
Post cath ECG: Now there are hyperacute T-waves again, and recurrent ST depression in V2 This ECG would normally diagnostic of OMI until proven otherwise No further troponins were measured, but it looks like there is recurrent OMI Next day: A CT CoronaryAngiogram was done (CTCA) CARDIAC MORPHOLOGY AND FUNCTION: 1. IMPRESSION: 1.
By the P s, Q s, 3 R Approach ( as reviewed in ECG Blog #185 ): The Q RS complex is obviously wide. CT coronaryangiogram — No obstructive coronary disease. CT coronaryangiogram showed no obstructive coronary disease. ECG Blog #185 — Systematic P s, Q s, 3 R Approach to Rhythm Interpretation.
Hospital evaluation for this patient was negative for an acute coronary syndrome ( ie, CT coronaryangiogram was normal — troponin was not elevated — and Echo was negative, with no sign of pericardial effusion ). See ECG Blog #215 — for more on the Cabrera format. = In contrast, the standard U.S.
Finally, do a coronaryangiogram Possible alternative to pacing is to give a beta-1 agonist to increase heart rate. For more on Torsades de Pointes vs PMVT See My Comment in the October 18, 2023 post and the September 2, 2024 post in Dr. Smith's ECG Blog ). Discontinue all QT proloning medications, including azithromycin 6.
A CT Coronaryangiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45 CAD-RADS category 1. --No
More cases can be found on the blog here. Here it is: So we looked for the followup: Cath lab was activated per protocol and coronaryangiogram found no angiographic significant obstructive disease in the LAD, LCX, and RCA. "Look how bizarre it is." When bizarre, look at leads I, II, and III. So I explained APTA to him.
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ).
Cardiology was consulted and the patient underwent coronaryangiogram which showed diffuse severe three-vessel disease. Coronaryangiogram shows diffuse severe three-vessel disease. Episodes of angina over past couple of months had been progressive. High sensitivity troponin I rose to peak at 2900 ng/L.
The post 6 Cardiology Board Review Questions That Will Help You Pass the Boards appeared first on BoardVitals Blog. Question banks are a favorite exam preparation resource for Cardiologists that want to practice in the format of the exam. If you’d like more sample questions then follow this link to begin a free trial today.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Edited by Smith He also sent me this great case.
Will you accept this patient for emergent coronaryangiogram based on the ECG changes? The patient is a 70 something female with chest discomfort and dyspnea. How would you interpret the ST changes seen in this ECG? Does the ECG represent STEMI-negative OMI findings? How would you mange this patient?
The patient was taken emergently to the cath lab for a pericardiocentesis instead of a coronaryangiogram. Regular readers of Dr. Smith's ECG Blog are well familiar with what is perhaps my favorite Stephen Smith Adage = "You diagnose acute pericarditis at your peril!"
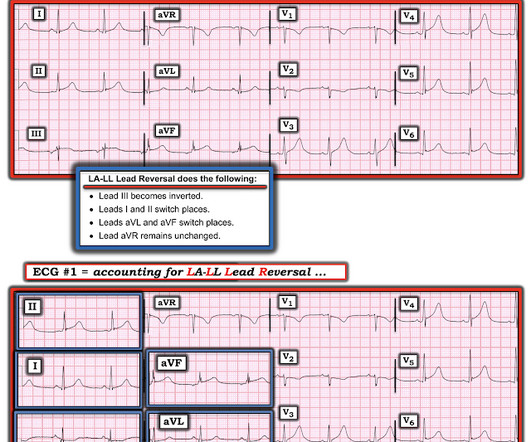
CT coronaryangiogram is excellent , but is rarely available outside of business hours, and hardly ever at night. In the July 28, 2020 post in Dr. Smith’s ECG Blog — I cited my favorite on-line “Quick GO-TO” reference for the most common types of lead misplacement, which comes from LITFL ( = L ife- I n- T he- F ast- L ane ).
Outcome The only followup we got was that the patient is undergoing Coronary Bypass (CABG) of LAD, 2nd Obtuse Marginal, and Left Posterolateral coronaries. We don't know if he had a stress test, a CT Coronaryangiogram, or they just decided to do an angiogram. But thanks to you, I feel much more confident.
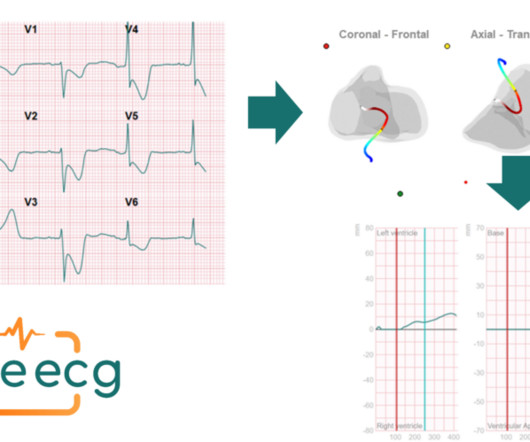
cineecg flow inferior wall infarct In this blog we will address a case of identifying a specific case of a heart infarct, in particular an infarct in the lower part of the heart (Inferior wall infarction ; RCA distal to the RV branch).
A Coronaryangiogram from 8 years prior revealed that he had had an inferior posterior STEMI at the time due to 100% occlusion of the proximal RCA. Regional wall motion abnormality- inferior and inferolateral.
Ct coronaryangiogram showed normal coronary arteries. Smith note: I think CT coronaryangiogram is reasonable with the elevated troponins and symptoms. He was given aspirin and heparin and transferred to the local cardiac center for further evaluation. He was diagnosed with mild AKI which resolved.
She had a prior history of "NSTEMI" one month ago, during which she had a coronaryangiogram reportedly showing no stenosis in any coronary artery. A very similar case to the one presented today appears in the January 17, 2023 post of Dr. Smith’s ECG Blog. Her vitals were within normal limits.
It’s judicious, then, to arrange for coronaryangiogram. Coronary occlusion, however, might be present concurrently with subendocardial ischemia on the time-zero ECG, or evolve into such. elevated BP), but rather directly correlated with coronary obstruction and stymied TIMI flow. Does the ECG normalize? 2] Aslanger, E.,
A coronaryangiogram was done that did not show significant coronary artery disease. I have periodically called attention to examples of the Ashman phenomenon as they occur in Dr. Smith's ECG Blog ( See My Comments in the January 5, 2020 post — the June 17, 2020 post — and the March 30, 2023 post , among others ).
Like they would for any other acute arterial occlusion syndrome (such as suspicion of acute large vessel stroke), they take the patient across the hall and perform an immediate CT (coronary) angiogram, showing patent coronaries. An emergent echo also confirms no regional wall motion abnormality.
We investigated the incidence of an acutely occluded coronary in patients presenting with STE-aVR with multi-lead ST depression. All electrocardiograms (ECGs) and coronaryangiograms were blindly analyzed by experienced cardiologists. A normal PR interval.
NSTEMI paradigm doesn't care if you have imminently deadly acute coronary occlusion, unless you have STEMI criteria, ongoing ischemia after hours of delay, or until you start to have shock or arrest from it. Just another NSTEMI.
Discussion Thus, no further ECGs were recorded and there was no angiogram or stress test or CT coronaryangiogram. Acute MI does not often present with syncope alone, without any other symptom, so the pretest probability of acute MI is low.
Here is the coronaryangiogram: A distal thrombotic right coronary artery (RCA) occlusion ! Cath lab was not activated because we diagnosed a "high risk" NSTEMI; rather, it was because we suspected, actively searched for, and could not refute an OMI that needs to be immediately reperfused.
Young people can suffer acute coronary occlusion, whether by typical atherosclerotic plaque rupture, or by coronary anomalies, coronary aneurysms, dissections, spasm, etc. The wall motion abnormalities of Takotsubo cardiomyopathy and LAD OMI can be similar.
The diagnostic coronaryangiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Aortic angiogram did not reveal aortic dissection. The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED.
See this exemplified many times on this blog. Heitner et al found that in 14% of patients with NSTEMI, a blinded interventional cardiologist interpreting coronaryangiograms identified a different culprit artery than CMR ( [link] ). Subendocardial ischemia does not localize. Anterior ST depression = posterior ST elevation.
Angiogram Door to balloon time was 120 minutes (much too long) because of time taken for a CT. Coronaryangiogram showed 100% mid LAD occlusion for which she received a DES with excellent angiographic result. It was not SCAD (coronary dissection) Highest troponin I was 37,000 ng/L, but it was not measured to peak.
The intricacies of the different classes of antiarrhythmics and their mechanism of action extend beyond the scope of this blog. CT coronaryangiogram showed a hypoplastic RCA and dominant LCx. I list below links to other cases of idiopathic VT from Dr Smith's ECG blog. Try a different kind of antiarrhythmic.
Case Continued The patient was discharged from the hospital with a plan for a scheduled coronaryangiogram to assess the coronary arteries and the possibility of aortic valve replacement. The vast majority of ischemia from supply demand mismatch is diffuse ST depression, with ST Elevation in aVR.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content