This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. The sinus tachycardia is a definite concern that something acute may be ongoing. Does the patient's age infuence your interpretation?
No chestpain. This leaves us with the usual differential diagnosis for this rhythm presentation ( as per ECG Blog #361 ) ==> We need to consider i ) VT until proven otherwise: ii ) SVT with either preexisting BBB or aberrant conduction; — or , iii ) Something else ( ie, WPW, hyperkalemia, some other toxicity, etc. ).
No clear history for recent chestpain — but the patient "has not been well" for the previous week. C linical I MPRESSION: I would interpret ECG #1 as suggestive of near ventricular standstill — with underlying atrial tachycardia, extended pauses, and no reliable ventricular escape focus. This is often a pre-lethal rhythm.
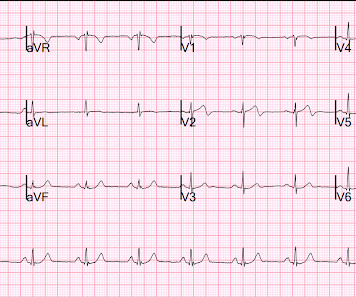
The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Continuing with assessment of ECG #1 in Figure-2: The rhythm is sinus tachycardia at ~110/minute. NOTE: Abnormal baseline deflections in Figure-2 are maximal i n leads I , II and aVR.
One reason why LBBB conduction in a patient with marked LVH may not evolve to a predominant ( if not all positive ) R wave by lead V6 — is that leftward and posterior forces of marked LVH with LBBB may delay transition to predominant positivity in the chest leads until more posteriorly oriented chest leads, such as V7 or V8.
I see the following: There is sinus tachycardia ( upright P wave with fixed PR interval in lead II ) — at the rapid rate of ~130/minute. See ECG Blog #435 — ECG Blog #313 — as well as My Comment at the bottom of the page in the June 17, 2024 post in Dr. Smith's ECG Blog ). Sinus tachycardia has resolved.
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. With normal EF the tachycardia is not compensatory.
Voltage for LVH is satisfied — at least by Peguero Criteria ( Sum of deepest S in any chest lead + S in V4 ≥23 mm in a woman — as discussed in ECG Blog #73 ). This point is particularly relevant regarding ECG #2 — because sinus tachycardia is seen on this earlier ECG. In the October 15, 2022 post of Dr. Smith's ECG Blog — Drs.
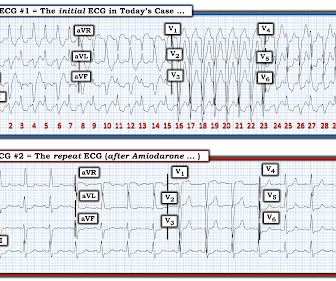
Easy LINKS — tinyurl.com/KG-ECG-Podcasts — [link] — Other ECG Audio PEARLS I previously made for my ECG Blog can be found in the right column of each page on this blog just below this icon — under, "ECG Audio PEARLS". Get a post -conversion 12-lead ECG — and compare this to the initial 12-lead ECG obtained during the tachycardia!
Written by Willy Frick A 67 year old man with a history of hypertension presented with three days of chestpain radiating to his back. Due to the chestpain radiating into the patient's back, the ER physician ordered CTA chest to rule out aortic dissection. He had associated nausea, vomiting, and dyspnea.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. This has been discussed many times before on this blog. Is there STEMI?
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). NOTE #1: Sinus tachycardia is not usually seen in an uncomplicated acute MI. All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation.
An elderly dialysis patient presented with chestpain. Here is her ECG: Regular Wide Complex Tachycardia. Here is her ECG: Regular Wide Complex Tachycardia. Could it be atrial tachycardia with RBBB and LPFB aberrancy? Here it is: There is sinus with normal conduction, very different from her tachycardia.
This was written by Magnus Nossen, from Norway, with comments and additions by Smith A 50 something smoker with no previous medical hx contacted EMS due to acute onset chestpain. Upon EMS arrival the patient appeared acutely ill and complained of chestpain. An ECG was recorded immediately and is shown below.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. There is sinus tachycardia at ~100/minute. Vitals were normal.
The ECG in Figure-1 was obtained from a 90-year old woman — who presented with a 2-to-3 day history of chestpain, that became worse on the day of admission. The terminology favored to describe these ECG findings is diffuse subendocardial ischemia ( See ECG Blog #271 — for more on diffuse subendocardial ischemia ).
He had concurrent sharp substernal chestpain that resolved, but palpitations continued. Over past 3 months, he has had similar intermittent episodes of sharp chestpain while running, but none at rest. Read this post: Idiopathic Ventricular Tachycardias for the EM Physician 2. Ken notes AV dissociation.
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. See these posts: ChestPain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab? What do you think?
Let me tell you about her hospitalization, discharged 1 day prior, but it was at another hospital (I wish I had the ECG from that hospitalization): The patient is 40 years old and presented to another hospital with chestpain and SOB. She had been sitting doing work when she experienced "waves of chest tightness". Sats were 88%.
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
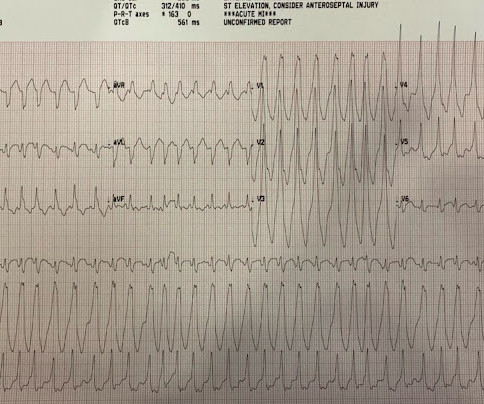
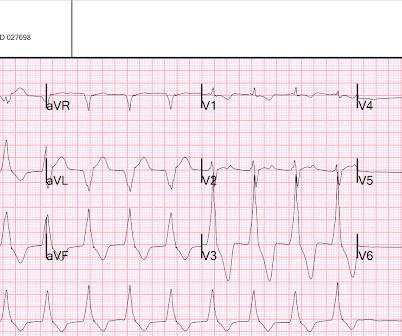
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. She presented to the emergency department after a couple of days of chest discomfort. Answer : The ECG above shows a regular wide complex tachycardia. Cardiac output (CO) was being maintained by the tachycardia.
He had no chestpain or shortness of breath. But it is not disorganized enough to be polymorphic ventricular tachycardia. Learning Points: Wide complex irregularly irregular tachycardias include PMVT, AF with WPW, and AF with aberrancy. See our other cases of AF with WPW: A young man with another episode of tachycardia.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. We can see enough to make out that the rhythm is sinus tachycardia. It was not worse with exertion or relieved by rest.
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. There is sinus tachycardia. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology.
Written by Bobby Nicholson MD and Pendell Meyers A man in his 30s presented to the ED for evaluation of chestpain and palpitations. The ECGs show a wide complex, irregularly irregular tachycardia. At this point, the patient had been symptomatic for almost 5 hours, appeared unwell with chestpain and diaphoresis.
The presenting complaint was chestpain — and the patient collapsed soon after arrival in the ED. The finding of a fairly regular, wide tachycardia without clear sign of atrial activity ( especially when seen in an acutely symptomatic patient ) — should immediately prompt a diagnosis of VT until proven otherwise.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. The Importance of the History: As noted above — the onset of chestpain in today's case was acute. He had received aspirin and nitroglycerin by EMS, with some improvement. His vitals were within normal limits.
No chestpain. Figure-1: The initial ECG in today's case — obtained from an 86-year old man with presyncope, but no chestpain. ( The Long Lead II Rhythm Strip: As always — I favor a systematic approach to rhythm interpretation, using the P s, Q s, 3 R memory aid ( See ECG Blog #185 ). What is the rhythm ?
By the P s, Q s, 3 R Approach ( as reviewed in ECG Blog #185 ): The Q RS complex is obviously wide. Given the rapid rate of the tachycardia and the amorphous shape of the QRS — the decision was made to sedate the patient and cardiovert. ECG Blog #185 — Systematic P s, Q s, 3 R Approach to Rhythm Interpretation.
The ECG in Figure-1 was obtained from an older woman — who presented with chestpain and palpitations over the previous hour. Contrast today's rhythm with true ventricular bigeminy — that was seen in ECG Blog #343 ). Contrast today's rhythm with true alternating bundle branch block — that was seen in ECG Blog #306 ).
Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? She had a very elevated troponin T at 12,335 ng/L at the time of presentation. The patient in today’s case suddenly became tachycardic while sleeping.
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
Sent by Dan Singer MD, written by Meyers, edits by Smith A man in his late 30s presented with acute chestpain and normal vitals except tachycardia at about 115 bpm. Dr. Singer sent this to me with just the information: "~40 year old with acute chestpain". Anxiety is a common cause of chestpain with tachycardia.
Just as important is pretest probability: did the patient report chestpain prior to collapse? Confirmation of sinus tachycardia should be easy to verify when the heart rate slows a little bit ( as the patient's condition improves ) — allowing clearer definition between the T and P waves. Then assume there is ACS.
The tachycardia was gone by the time paramedics arrived. But syncope or seizure alone, without chestpain, is not enough to call it Wellens syndrome. Without chestpain, the pretest probability is not very high. With the chestpain history, this is now Wellens' syndrome. There was tongue biting.
This one is far more specific, as it is combined with sinus tachycardia and some T-wave inversion in V1-V3. and tachycardia, 1.8. Finally , they found that S1Q3T3, precordial T-wave inversions V1-V4, and tachycardia were independent predictors of PE. This is a classic S1Q3T3. Most S1Q3T3 is not due to PE. incomplete RBBB 1.7
PEARL # 6: As I discuss in my review of SSS ( See ECG Blog #342 for details ) — establishing a diagnosis that sinus bradycardia indicates SSS — will depend on the following: Finding out the age of the patient ( ie, SSS is most common in older individuals ) — and learning whether the patient has been symptomatic? ( No pause beyond 2.0
CT of chest showed the bullet path through his right lung but nowhere near his heart. There were times when it would be usurped by sinus tachycardia, then return to this rhythm. But he did get an EKG: What is this? There is a wide complex. It is irregular. It is not fast (cannot be VT).
Here is his ECG: Original image, suboptimal quality Quality improved with PM Cardio digitization The ECG is highly suggestive of acute right heart strain, with sinus tachycardia, S1Q3T3, and T wave inversions in anterior and inferior with morphology consistent with acute right heart strain. Moreover, there is tachycardia.
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". He mentioned "cancer" and "chest". There is a narrow complex tachycardia at a rate of 130. He was awake, with a pulse of 130 and BP of 50/30. Is is sinus?
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content