This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
As discussed in detail in ECG Blog #228 — this seemingly qualifies as a “ Silent ” MI ( Approximately half of those MIs not accompanied by CP — have some other associated symptom such as syncope, which substitutes as a “chestpain equivalent” ). Smith's ECG Blog ). What is T-QRS-D? This is not the case.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think? This was the cost of preventing infarction of the anterior wall.)
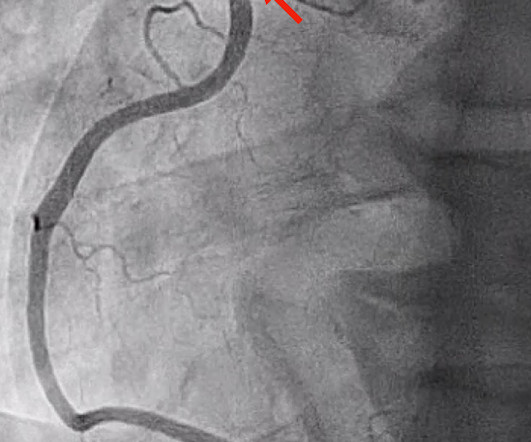
He did not remember whether he had experienced any chestpain. His ECG at the accepting facility is shown below: Accepting facility ECG The team reviewed his angiography films with an interventionalist and thought they were suspicious for plaque rupture in LAD, but they were not confident. He was admitted to cardiology.
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The pathologist may see a plaque that constitutes, for example, 50% of the cross-sectional area.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
Sent by Drew Williams, written by Pendell Meyers A man in his 50s with history of hypertension was standing at the bus stop when he developed sudden onset severe pressure-like chestpain radiating to his neck and right arm, associated with dyspnea, diaphoresis, and presyncope. EMS arrived and administered aspirin and nitroglycerin.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A previously healthy middle-aged male presented shortly after the acute onset of chestpain very shortly before calling 911. On arrival, he was pain free: What do you think? Jerry Jones commented: "Any ST depression on the ECG of a patient with chestpain credible for ACS represents a reciprocal change until proved otherwise."
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." A similar episode had occurred a week earlier during labor.
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
This is a previously healthy male teenager who was awoken by chestpain. The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chestpain.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion). Is there STEMI?
He also complained of intermittent mild chestpain radiating into into both shoulders and his back, as well as occasional unexplained sweating. ECG 1 Readers of this blog will have no trouble recognizing this as an OMI with some early reperfusion. He had no further chestpain. < 0.033). His ECG is shown.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
A 20-something male presented from an outside facility with Chestpain. He came with this ECG from the outside facility, recorded 1 hour after pain onset: There is at least 2 mm of inferior ST elevation, with reciprocal ST depression in aVL, ST flattening in V4-V6, and T-wave inversion in V2. Vital signs were normal.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
The patient said his chestpain was 4/10, down from 8/10 on presentation. Although it is statistically unlikely, multiple plaque ruptures are possible. The PDA plaque was also bulky, but was not described as inflamed or ulcerated. The PDA plaque was also bulky, but was not described as inflamed or ulcerated.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. There are multiple possible clinical situations that could account for diffuse subendocardial ischemia that is not due to ACS and plaque rupture. The syncope lasted about 2-3 minutes according to his wife.
Here is the clinical story: A 40 year old male with no cardiac history presented with acute substernal chestpain that started 40 minutes prior to arrival. In spite of a relatively short QTc of 376 ms, the very low R-wave amplitude in V4 and the ST Elevation at 60 ms after the J-point in lead V3 contribute to a high final value.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Written by Willy Frick A 40 year old woman was at home cooking when she developed chestpain. Smith comment : a very high proportion of MINOCA are ruptured plaque with lysed thrombus. That plaque is at risk of thrombosing again. An angiogram is a " lumenogram " and does not "see" the extraluminal plaque.
Cardiology Board Review Question A 48-year-old female with no known medical history presents with acute substernal chestpain. Patients typically present with acute chestpain, shortness of breath, or syncope. The most common presenting symptom is acute substernal chestpain. What are the Symptoms?
Because: 1) He has been reading this blog for a long time. Case A 43 year old male with a history of DM II, hyperlipidemia, and a family history of myocardial infarction presented to a family clinic with two days of epigastric pain that started after consuming a meal. A chest x-ray in the ED found bilateral pleural effusions.
In this blog, well explore why anemia can occur after heart bypass surgery, how common it is, and how it can be managed. This condition occurs when the blood vessels that supply blood to the heart become blocked or narrowed by plaque buildup. It can also be considered a postoperative complications may hinder recovery.
Case A 42-year-old lady presented to the ED with complaints of intermittent episodes of chestpain associated with shortness of breath for the last 2 days. This was her ECG (it is unclear if this was with or without pain): Computerized ECG Read: “Normal sinus rhythm. This case was written by Sam Ghali: ( @EM_RESUS ). Normal ECG.”
In this blog, we’ll break down the steps of coronary circulation, helping you understand how your heart maintains its own health while keeping the rest of the body alive and well. Angina : This is chestpain caused by reduced blood flow to the heart muscle, often triggered by physical exertion or stress.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
She asked me why I felt she had had a heart attack and I explained to her that she had had chestpains and the blood test indicating damage to the heart was elevated and that was all we needed to say that she had had a heart attack. On the basis of these findings we told her that she had suffered a heart attack.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. Chestpain, SOB, Precordial T-wave inversions, and positive troponin. What is the Diagnosis? Now another, with ultrasound.
Here is a case of an 89 year old woman who had syncope but no chestpain or shortness of breath. There was a ruptured plaque with thrombus in the LAD, with some flow still (accounting for the inverted T waves). Her initial EKG (#1) shows some ST depression in V4-V6, possibly ischemic or possibly due to LVH.
A 40-something woman had sudden chestpain. Today, they viewed the angiogram and concluded that the thrombus at the mid RCA must have extended proximally from the culprit ruptured plaque, extending proximal to the RV marginal branch and temporarily occluding it. She called 911. But which myocardial walls are affected?
He did not state he had chestpain, but, then again, he couldn't remember anything. The ECG and ultrasound could not have been differentiated from acute plaque rupture with occlusion of the RCA. This 80 year old with a history of CABG had a cardiac arrest. There is concordant ST elevation in all inferior leads.
High cholesterol levels – Elevated levels of bad cholesterol can contribute to plaque buildup in your arteries, increasing the risk of heart disease. Routine blood pressure checks are essential to maintaining a healthy heart as high blood pressure often has no symptoms.
The chief complaint was "chestpain." Male patient: I went back to the room of the first patient and he stated that he had been having chestpain on and off for 3 days. It was actually a dissection, not an atherosclerotic plaque rupture. Two Cases Male Patient I was handed this ECG of a 40-something male patient.
Acute MI due to plaque rupture does happen in young people, including young women. Instead, in a patient with new chestpain and hyperacute inferior lead T waves — this picture that we see in lead V3 suggests associated posterior OMI until proven otherwise. Beware a low HEART score.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. A normal PR interval.
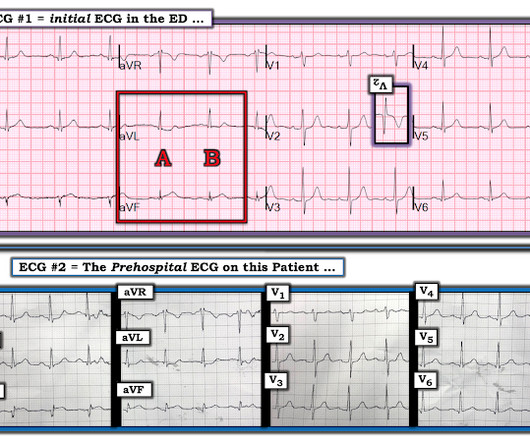
While ST coving in V1 is not necessarily abnormal — the presence of ST elevation in association with ST-T wave abnormalities in V2,V3 in a patient with chestpain is clearly cause for concern. Given that chestpain is resolving at the time ECG #2 was recorded — this supports the concept of dynamic ST-T wave changes in this patient.
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. As there was ruptured plaque, this is NOT Prinzmetal's angina. It is just as dangerous, as there is a ruptured plaque with thrombus (which lysed) in the proximal LAD. Values: STE60V3 = 2.0, QRS V2 = 10, RAV4 = 15.5, There was good flow. It was stented.
FYI : 52 ng/L is the threshold for "rule in" by European studies as it has a high positive predictive value in the setting of chestpain. Case continued The patient was placed on a nitroglycerin drip and chestpain gradually resolved. Top right is colored iodine overlay; Blue areas of myocardium are ischemia.
She was treated medically for NonSTEMI, pending next day cath, which showed ulcerated plaque and a 60% thrombotic stenosis in the LAD distal to the first diagonal. Serial ECGs correlated to the presence ( and severity ) of chestpain — often reveal the status of the "culprit" artery (ie, occluded, reopened, reoccluded ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content