This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
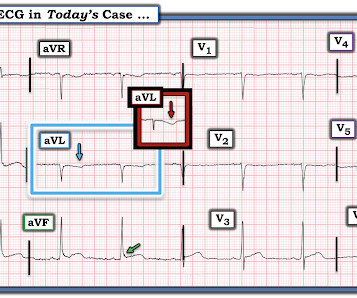
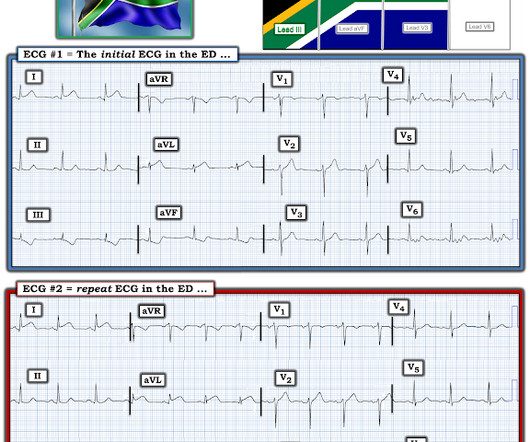
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. Does the patient's age infuence your interpretation? Figure-1: The initial ECG in today's case. ( Figure-2: I've labeled t he initial ECG.
In this ECG Cases blog, Jesse McLaren and Rajiv Thavanathan explore how ECG and POCUS complement each other for patients presenting to the emergency department with shortness of breath or chestpain. The post ECG Cases 49 – ECG and POCUS for Dyspnea and ChestPain appeared first on Emergency Medicine Cases.
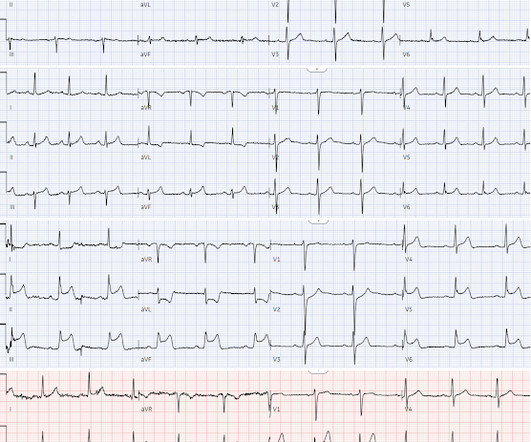
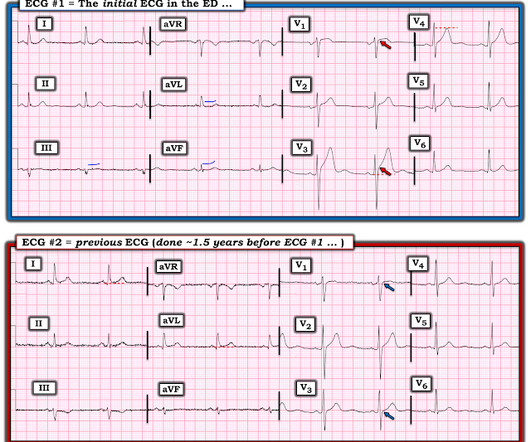
For full discussion of this case — See ECG Blog #292 — == The 2 ECGs shown in Figure-1 were obtained from a man in his 30s — who presented to the ED ( E mergency D epartment ) with chestpain that began several hours earlier. ECG Blog #260 — Reviews another case that illustrates the concept of "dynamic" ST-T wave changes.
No clear history for recent chestpain — but the patient "has not been well" for the previous week. I review my user-friendly approach to the ECG diagnosis of the Bundle Branch Blocks in ECG Blog #282 — and to Hemiblocks and Bifascicular Blocks in ECG Blog #203. ECG Blog #394 — reviews another case of Masquerading BBB.
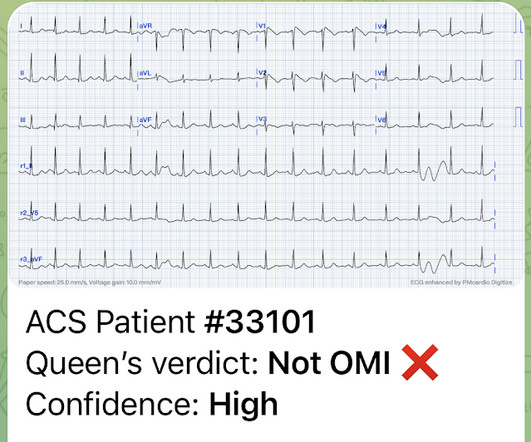
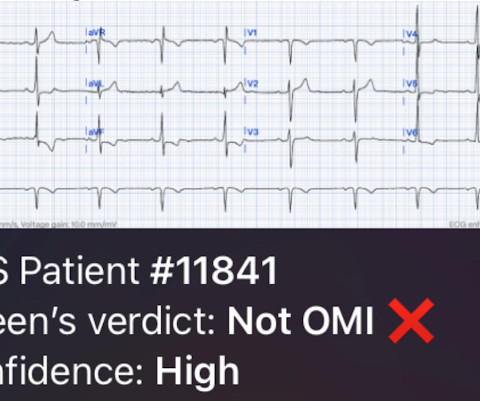
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
No chestpain. This leaves us with the usual differential diagnosis for this rhythm presentation ( as per ECG Blog #361 ) ==> We need to consider i ) VT until proven otherwise: ii ) SVT with either preexisting BBB or aberrant conduction; — or , iii ) Something else ( ie, WPW, hyperkalemia, some other toxicity, etc. ).
This was sent by anonymous The patient is a 55-year-old male who presented to the emergency department after approximately 3 to 4 days of intermittent central boring chestpain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
Of course he said: "Yes, it was a 60 year old diabetic with Chestpain." More cases can be found on the blog here. As per Dr. Smith — I review in detail the mathematical relationships seen when there is APTA in one of the extremities in My Comment in the January 17, 2023 post of Dr. Smith's ECG Blog. That is not a STEMI.
I assumed it was a patient with acute chestpain. It was a man in his 30s with chestpain. While statistical likelihood of acute OMI is clearly lower in younger adults — nothing is ruled out by age alone ( as per My Comment in the January 9, 2023 and December 5, 2023 posts in Dr. Smith's ECG Blog ). 27 post ).
One reason why LBBB conduction in a patient with marked LVH may not evolve to a predominant ( if not all positive ) R wave by lead V6 — is that leftward and posterior forces of marked LVH with LBBB may delay transition to predominant positivity in the chest leads until more posteriorly oriented chest leads, such as V7 or V8.
As discussed in many posts in this ECG Blog — despite not satisfying the millimeter-based definition of a STEMI — in this patient with new chestpain, the ECG findings in Figure-1 merit prompt cath lab activation without any need to wait for serum troponin to return elevated ( See ECG Blog #193 — regarding the new "OMI" paradigm ).
KEY Point: Although true that patients with longstanding, severe pulmonary disease may manifest a QRST complex in standard lead I with marked overall reduction in QRST amplitude ( See ECG Blog #65 — regarding Schamroth’s Sign ) — you should never normally see a completely flat line in any of the standard limb leads.
I i llustrate the ECG finding of T-QRS-D below in Figure-3 , which I've excerpted from My Comment in the November 14, 2019 post in Dr. Smith's ECG Blog. Today's case is also noteworthy in that T-QRS-D is seen in association with RBBB — which has only been described on rare occasions ( See the March 28, 2021 post i n Dr. Smith's ECG Blog ).
Written by Jesse McLaren A 45-year-old presented with 24 hours of intermittent chestpain. On it’s own this is nonspecific, but in the right context this could be diagonal occlusion (if active chestpain) or infero-posterior reperfusion (if resolved chestpain). #2 Can you guess the sequence?
For full discussion of this case — See ECG Blog #392 — == The ECG in Figure-1 was obtained from a man in his 60s — who described the sudden onset of "chest tightness" that began 20 minutes earlier, but who now ( at the time this ECG was recorded ) — was no longer having symptoms. ECG Blog #387 — Dynamic change in 2 minutes.
and , ii ) That we need to carefully inquire about recent chestpain, paying special attention to the rest of this 12-lead ECG ( looking carefully for signs of acute or recent infarction — because AV Wenckebach is common with acute inferior MI ). ECG Blog #205 — Reviews my System for 12-Lead ECG Interpretation.
Written by Pendell Meyers Two patients with acute chestpain. Patient 1: Patient 2: Patient 1: A man in his 40s with minimal medical history presented with acute chestpain radiating to his R shoulder. Two patients with chestpain. Do either, neither, or both have OMI and need reperfusion?
For more regarding ECG criteria for LVH — See the ADDENDUM below and/or ECG Blog #73 and ECG Blog #245. BOTTOM Line: Today's patient presented with a 2-3 day history of chestpain and the ECG shown in Figure-1. ECG Blog #245 — Reviews the ECG diagnosis of LVH.
As discussed in detail in ECG Blog #228 — this seemingly qualifies as a “ Silent ” MI ( Approximately half of those MIs not accompanied by CP — have some other associated symptom such as syncope, which substitutes as a “chestpain equivalent” ). ECG Blog #218 — Reviews HOW to define a T wave as being H yperacute ?
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. Inferior hyperacute T waves, which have been added to the 2022 ACC consensus on chestpain as a “STEMI equivalent”[3] 3. But are there any other signs of Occlusion MI? Conduction disorders in the setting of acute STEMI.
Voltage for LVH is satisfied — at least by Peguero Criteria ( Sum of deepest S in any chest lead + S in V4 ≥23 mm in a woman — as discussed in ECG Blog #73 ). In the October 15, 2022 post of Dr. Smith's ECG Blog — Drs. Intervals ( PR, QRS and the QTc ) and the frontal plane axis are normal. What is P recordial S wirl ?
She was hemodynamically stable — and did not have chestpain, lightheadedness or syncope. To do this — I apply the P s, Q s, 3 R Approach ( See ECG Blog #185 — for review of my system ). R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation.
See ECG Blog #435 — ECG Blog #313 — as well as My Comment at the bottom of the page in the June 17, 2024 post in Dr. Smith's ECG Blog ). Today’s patient presented to the ED not only with chestpain — but also with shortness of breath , therefore with a history potentially consistent with the diagnosis.
By the P s, Q s, 3 R Approach ( which I review in ECG Blog #185 ): Lots of P waves are present — being well seen in the long lead II rhythm strip. This slight variation in sinus P wave regularity tends to be greater when a 2nd- or 3rd-degree AV block is present ( called ventriculophasic sinus arrhythmia — as shown in ECG Blog #344 ).
A 50-something male had onset of chestpain 1 hour prior to ED arrival. Endorses some associated SOB, but denies back pain, fever, cough, chills, leg swelling, or other new symptoms. Always get serial ECGs in a patient with acute chestpain. It is constant, 9/10, left-sided CP that radiates into left arm and jaw.
A young woman presented with acute chestpain. This case came from a friend whose sister was the patient. She knew I was interested in ECGs, so she took a photo of this one. This was her presenting ECG: What do you think? This is clearly Brugada phenotype. There is downsloping ST Elevation in V1 and V2.
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. How would you assess this ECG? What is your next step?
The patient was a middle-aged female who had acute chestpain of approximately 6 hours duration. The pain was still active at the time of evaluation. See some relevant cases below: Chestpain with anterior ST depression: look what happens if you use posterior leads.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. This has been discussed many times before on this blog. Is there STEMI?
Written by Pendell Meyers A man in his 60s presented with acute chestpain and normal vital signs. Here is his triage ECG: What do you think? The ECG shows massively hyperacute T waves of LAD OMI, plus WPW. V3-V5 also have the depressed HATW takeoff which qualifies them as the rare de Winter subtype of HATWs.
Easy LINKS — tinyurl.com/KG-ECG-Podcasts — [link] — Other ECG Audio PEARLS I previously made for my ECG Blog can be found in the right column of each page on this blog just below this icon — under, "ECG Audio PEARLS". I recently recorded a series of 4 podcasts regarding KEY concepts in ECG interpretation.
A 50 year old presented to the emergency department of a remote rural community (where the nearest cath lab is a plane ride away) with one hour of mild chestpain radiating to the back and jaw, and an ECG labeled ‘normal’ by the computer interpretation. What do you think, and how would you manage the patient?
Written by Jesse McLaren A 45 year old presented with two weeks of recurring non-exertional chestpain, now constant for an hour. Because of the ECG changes in a patient with chestpain, and with inferolateral hypokinesis on POCUS, the cath lab was activated. Below is old and then new ECG (old on top; new below).
As reviewed in ECG Blog #350 — t he clinical significance of Wellens' Syndrome — is that its recognition tells you that the patient has a high-grade LAD narrowing with presumably "hot" thrombus h avin g high propensity to propagate and/or totally occlude the LAD at any point in time ( including immediately ). What is W ellens’ S yndrome ?
Written by Willy Frick A man in his early 40s with BMI 36, hypertension, and a 30 pack-year smoking history presented with three days of chestpain. He described it as a mild intensity, nagging pain on the right side of his chest with nausea and dyspnea. It started while he was at rest after finishing a workout.
Written by Willy Frick A 67 year old man with a history of hypertension presented with three days of chestpain radiating to his back. Due to the chestpain radiating into the patient's back, the ER physician ordered CTA chest to rule out aortic dissection. He had associated nausea, vomiting, and dyspnea.
A 56 year old male with PMHx significant for hypertension had chestpain for several hours, then presented to the ED in the middle of the night. He reported chestpain that developed several hours prior to arrival and was 5/10 in intensity. The pain was located in the mid to left chest and developed after riding his bike.
Written by Pendell Meyers A man in his 40s called EMS for acute chestpain that awoke him from sleep, along with nausea and shortness of breath. His history included known heart failure with prior EF 18%, insulin dependent diabetes, and polysubstance abuse. Vitals were within normal limits except for tachypnea.
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
This was sent by Sam Ghali @EM_RESUS A 44 year old man presented with chestpain The tech came running with the ECG as the computer called "STEMI!" What do you think? Sam sent this to me and asked: "What do you think, Steve?" My answer: --Tough one! --But
Sent by Magnus Nossen MD, written by Pendell Meyers A man in his 50s, previously healthy, developed acute chestpain. The primary care physician there evaluated this patient and deemed the chestpain to be due to gastrointestinal causes. The ECG was also interpreted as normal by the primary care physician.
He did not remember whether he had experienced any chestpain. The electrophysiologist is a reader of Dr. Smith's ECG Blog. The above said — it may prove insightful to take another look at the Wellens' Syndrome case instantly recognized by Dr. Smith in the August 12, 2022 post in Dr. Smith’s ECG Blog.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content