This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
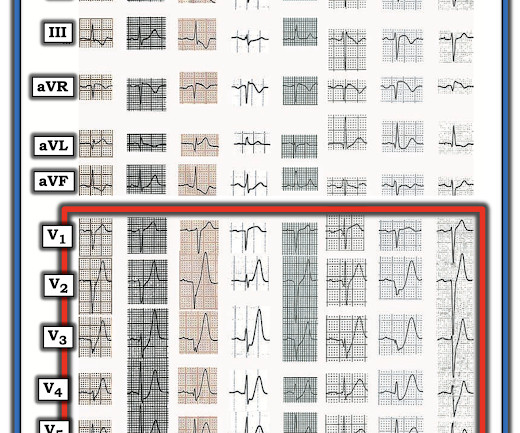
A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenicshock. Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. Referring to Figure-1 — this 53-year old woman who presented in extremis with cardiogenicshock and an initial pH = 6.9,
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). Today's patient did make it to the hospital — but was in cardiogenicshock, and despite valiant attempt at treatment, succumbed soon after.
The VSR is what is causing the cardiogenicshock! Another possible cause of pseudonormalization of T waves mentioned many times on this blog is the pseudonormalization caused by re-occlusion of an infarct related reperfused coronary artery. PIRP is strongly associated with myocardial rupture. Below are two more video files.
Now appears to be in cardiogenicshock." This is ischemia until proven otherwise. However, cardiogenicshock usually takes some time to develop, so it is probably subacute." Cardiogenicshock and ACS is an indication for the cath lab, even if you don't think there is OMI. I was texted these ECGs.
The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. There is no definite evidence of acute ischemia. (ie, Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. (
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenicshock" is not applicable outside of sinus rhythm. In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished.
ACS and STEMI generally do not cause tachycardia unless there is cardiogenicshock. Then ACS (STEMI) might be primary; this might be cardiogenicshock. Even if this ECG is the first thing one sees (as it was for me), one should stop and think: "This is an unusual STEMI." Are the lungs clear? Is the patient cool and pale?
Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. The patient died of cardiogenicshock within 24 hours despite mechanical circulatory support. There are also J-waves.
Contrary to what Ken stated, the ST vector remains mostly posterior __ What about subendocardial ischemia? Subendocardial ischemia results in ST depression, but unfortunately, and rather mysteriously, it does not localize to the ischemic wall. Similarly, STD in aVL is usually reciprocal to inferior ST elevation, not "lateral ischemia."
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern). The patient arrived to the ED in cardiogenicshock but awake.
There is normal R-wave progression in the precordial leads with no evidence of ischemia. Here the image quality is enhanced using the PM Cardio app. What do you think? The presenting ECG shows SR with narrow QRS complexes. In the limb leads there is T-wave inversion in lead aVL with a low amplitude QRS preceding the T-wave.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. So there is now high pre-test probability + refractory ischemia + Modified Sgarbossa + dynamic ECG changes. But by this time the patient went into cardiogenicshock and passed away.
My most talented blog readers are paramedics because they have to put themselves on the line every time they activate the cath lab. Then the notes mention "cardiogenicshock" but without any reference to a cardiac echo or to a chest x-ray. This is the etiology of the syncope and hypotension and shock and elevated CVP.
The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. The patient is started on epinephrine infusion for cardiogenicshock and cardiology took the patient to the cath lab. The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria.
All of this appears to be consistent with "No Reflow", or small vessel occlusion with persistent ischemia in spite of an open artery. His included cardiogenicshock, V Tach, AV block. --There is persistent ST elevation in leads V1-V4, with a lot of STE in V4 (another bad sign). Such large infarcts have many complications.
Assessment was severe sudden cardiogenicshock. Use of objective evidence of myocardial ischemia to facilitate the diagnostic and prognostic distinction between type 2 myocardial infarction and myocardial injury. Clinically — the patient was felt to be in cardiogenicshock. They recorded an EC G: New ST Elevation.
Why is the patient in shock? He was in profound cardiogenicshock. RCA ischemia often results in sinus bradycardia from vagal reflex or ischemia of the sinus node. There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1.
This strongly suggests reperfusing RCA ischemia. Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. were pretty sick, with mostly LM/pLAD lesions and high rates of cardiogenicshock. Lobo et al.
Impella (cardiac output augmentation device) placed for cardiogenicshock Unfortunately, the patient progressed to multiorgan failure with worsening cardiac output despite being maxed on pressors and a balloon pump. EKG shown here: LAFB with no clear signs of OMI or ischemia. He expired 4 days later. No labs were performed.
The patient went into cardiogenicshock and ultimately died of this MI. Given our concern about possible subtle high-lateral OMI — this raises the question whether the upright T waves in leads V1 and V2 of this 1st ECG might be abnormal and reflect ischemia. Regional WMA: Lateral , large, hypokinetic.
The ECG shows sinus tachycardia, RBBB+LAFB, and signs of anterolateral acute transmural ischemia (most likely due to acute coronary occlusion), with concordant STE in I and aVL, inappropriate STE in V4-6 (though limited a bit by motion, still definite). Near 100% mortality without rapid reperfusion." The ST Elevation is NOT typical.
Whenever there is tachycardia, I am skeptical of OMI unless it has led to severely compromised ejection fracction with cardiogenicshock. The patient was started on heparin for possible NSTEMI vs demand ischemia. increasing stenosis, ischemia, volume changes, increased blood pressure, atrial fibrillation, etc.)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content