This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
See ECG Blog #435 — ECG Blog #313 — as well as My Comment at the bottom of the page in the June 17, 2024 post in Dr. Smith's ECG Blog ). PEARL # 2: In the absence of associated heart failure ( cardiogenicshock ) — sinus tachycardia is not a common finding in acute MI.
A 20-something presented after a huge verapamil overdose in cardiogenicshock. This was a very complex case and the details are too much for an ECG Blog, but suffice it to say that, s hortly thereafter, the patient had an asystolic arrest and was resuscitated. The initial K was 3.0 mEq/L and ionized calcium was 5.5
As reviewed in ECG Blog #350 — t he clinical significance of Wellens' Syndrome — is that its recognition tells you that the patient has a high-grade LAD narrowing with presumably "hot" thrombus h avin g high propensity to propagate and/or totally occlude the LAD at any point in time ( including immediately ). What is W ellens’ S yndrome ?
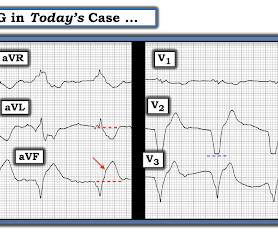
A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenicshock. Referring to Figure-1 — this 53-year old woman who presented in extremis with cardiogenicshock and an initial pH = 6.9, This was sent by a reader. and K was normal. Here was the ECG: There is sinus tachycardia.
Figure B At this point, with the ECG changing from diffuse ST depression to widespread ST elevation and the patient presenting in cardiogenicshock, left main coronary artery (LMCA) occlusion is the likely diagnosis. And then, 15 minutes later in today's case — this patient was in cardiogenicshock.
Now appears to be in cardiogenicshock." However, cardiogenicshock usually takes some time to develop, so it is probably subacute." Cardiogenicshock and ACS is an indication for the cath lab, even if you don't think there is OMI. I was texted these ECGs. Then SOB and nausea the next day.
The VSR is what is causing the cardiogenicshock! Another possible cause of pseudonormalization of T waves mentioned many times on this blog is the pseudonormalization caused by re-occlusion of an infarct related reperfused coronary artery. PIRP is strongly associated with myocardial rupture. Below are two more video files.
Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenicshock). As per Dr. Frick — sinus tachycardia is usually not seen with acute OMI unless the patient is in cardiogenicshock. Additionally, there is borderline right axis deviation. Both were wrong.
Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiac arrest, cardiogenicshock or impending shock. Today's patient did make it to the hospital — but was in cardiogenicshock, and despite valiant attempt at treatment, succumbed soon after.
The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. As we've often emphasized on Dr. Smith's ECG Blog — it is rare in practice to see LMCA occlusion, because most such patients die before reaching the hospital. RCA — 100% proximal occlussion.
The post Top 10 of 2022 – EM Cases Podcasts & Blogs Highlights of the Year appeared first on Emergency Medicine Cases. Based on a blend of number of listens, feedback from listeners, website visits and my personal faves, here is EM Cases Top 10 of 2022.
Heparin bolus (4000u), infusion Plan for rate control 25 mg IV diltiazem given HR = 143 25 mg IV repeat dose diltiazem given HR = 143 Diltiazem drip 10 mg/ hr for ~20 min HR remained 140 - 155 Then the patient developed Cardiogenicshock and echo had poor contractility Amiodarone load given. Patient intubated.
Here is the Queen of Hearts (version 1) interpretation: Click here to sign up for Queen of Hearts Access Angiogram images before and after intervention: Another view (before and after intervention): The patient was confirmed to be in cardiogenicshock, placed on ECMO, also with impella assist device.
ACS and STEMI generally do not cause tachycardia unless there is cardiogenicshock. Then ACS (STEMI) might be primary; this might be cardiogenicshock. Even if this ECG is the first thing one sees (as it was for me), one should stop and think: "This is an unusual STEMI." Are the lungs clear? Is the patient cool and pale?
He was in cardiogenicshock. The patient died 8 hours later of cardiogenicshock. Here are more examples of wide complex tachycardia: these are all a mix of ventricular tachycardia and SVT with aberrancy. This 51 yo male complained of chest pain, then had a v fib arrest. There is tachycardia, and there is a wide complex.
A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenicshock. For more on Precordial Swirl — See the October 15, 2022 post in Dr. Smith's ECG Blog ). She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. She could not be resuscitated.
The notes now refer to the patient being in cardiogenicshock, on pressors. hours from presentation, where he was found to have an acute thrombotic LAD occlusion which was stented with resulting TIMI 3 flow, but still the patient was in severe cardiogenicshock. Time = 3 hours: the next troponin returns at 60 ng/L.
She arrived comatose and in cardiogenicshock and the following ECG was recorded. Before EMS arrived, she had "seizure activity" and became unresponsive. She was defibrillated successfully from ventricular fibrillation and developed a perfusing rhythm. She was intubated.
The patient died of cardiogenicshock: Go to the post to see the full explanation. These were catastrophically missed (EM cath lab activation cancelled both times by the interventionalist) Here is a case of Sinus with RBBB and LAFB that was diagnosed correctly by the emergency physicians as acute STEMI.
Authors' commentary: Cardiogenicshock in the setting of severe aortic stenosis. This patient’s severe aortic stenosis (AS) and associated severe cardiogenicshock likely created the ECG pattern, resulting in a very difficult challenge for our inpatient team. If you can use Doppler, then you can diagnose it. Circulation.
Smith : LAD OMI with RBBB/LAFB is not only subtle on the ECG, but most of these patients are extremely ill: most I have seen are post-ROSC, in cardiogenicshock, or arrested shortly after.
Tachycardia is unusual for OMI, unless the patient is in cardiogenicshock (or getting close). ECG 2 Especially in the context of the first ECG, readers of this blog will readily appreciate the ST elevations and hyperacute T waves in II, III, aVF, V6, and to a lesser extent V5. link] I also texted the ECG to Dr. Smith.
I’m an avid reader of your blog, and wanted your valued opinion on this. He went into cardiogenicshock and is intubated in the cardiac ICU. Both the patient and his wife attributed it to spicy food a couple hours prior, and I had to talk him in to being transported. Cortland : Thank you so much for your reply!
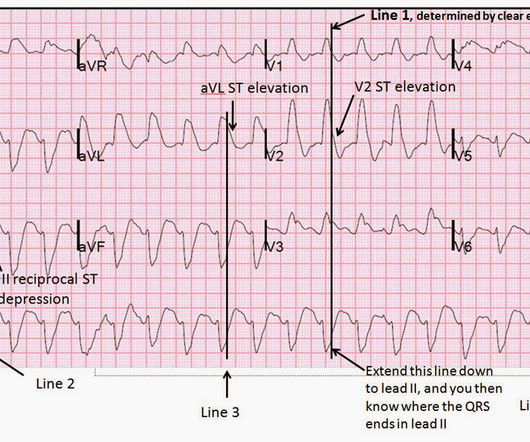
This pattern is essentially always accompanied by cardiogenicshock and high rates of VT/VF arrest, etc. The patient arrived to the ED in cardiogenicshock but awake. With so much STD in leftward and inferior leads V4-V6, II, III, and aVF, of course there must be STE in aVR. Code STEMI was activated.
As physicians, we know the value of placing a hand on someone’s calf, detecting a subtle drop in body temperature, and knowing that they have decompensated into a low output cardiogenicshock. Yet, not every patient or situation requires in person care — and those visits can be avoidably wasteful in time, effort, and cost.
Smith's book : Learning points: 1) OMI can be very subtle and RV infarction may manifest poorly on the standard ECG. 2) Typical persistent chest pain with a sigificantly elevated troponin is OMI until proven otherwise, regardless of the ECG. Our THANKS to Dr. Magnus Nossen for sharing this case with us.
OTHER Examples of Lead Reversal on Dr. Smith's Blog: Technical errors featuring a variety of lead reversal placements remain a surprisingly common “mishap” of everyday practice. The virtually identical QRST morphology in the limb leads between these 2 tracings confirms that there was LA-RA Lead Reversal in ECG #2a.
The patient died of cardiogenicshock within 24 hours despite mechanical circulatory support. The axis is to the right and QRS complexes in lead I and aVL are predominantly negative suggesting LPFB. This patient at cath had a large CX occlusion with a massive troponin release. Troponin T >42.000ng/L.
My most talented blog readers are paramedics because they have to put themselves on the line every time they activate the cath lab. Then the notes mention "cardiogenicshock" but without any reference to a cardiac echo or to a chest x-ray. And they teach me a lot. Was there pulmonary edema? Not mentioned in physicians' notes.
Among others — See My Comment at the bottom of the page in the September 13, 2024 post of Dr. Smith's ECG Blog ). As often emphasized by Dr. Smith — sinus tachycardia is not a common finding with acute OMI unless something else is going on (ie, cardiogenicshock ). Patient # 1: The "Tricky" Findings in the Initial ECG.
His included cardiogenicshock, V Tach, AV block. This poor echo can be seen even after very good reperfusion because myocardium that is still viable can be "stunned" and take weeks to recover. But the ECG is telling us that the myocardium will probably not recover. Such large infarcts have many complications.
Assessment was severe sudden cardiogenicshock. NOTE: For those interested — I review in detail determination of the artifact “culprit extremity” in My Comment in the September 27, 2019 post of Dr. Smith’s ECG Blog. Clinically — the patient was felt to be in cardiogenicshock. What is it? There is STE in V2-V6.
Because of the tachcardia, I would expect her to be very poor left ventricular function and maybe Cardiogenicshock. For another example of intermittent RBBB conduction, in which a similar initial deflection with terminal delay facilitated recognition of RBBB Conduction — Please SEE the June 25, 2020 post in Dr. Smith's Blog.
Just prior to transport, the patient became confused and agitated and, although blood pressure and pulse were OK, I was worried about cardiogenicshock. Diagnosis : Posterior MI, right? We intubated him. Cath lab The BP was 70/40 on arrival to the cath lab and received a balloon pump and norepinephrine.
He was in cardiogenicshock requiring an impella for several days after cath. We've shown many cases on Dr. Smith's ECG Blog of subtle ECG findings that rapidly evolve into dramatic ST-T wave changes. No further troponins were measured. But we should not be surprised.
Why is the patient in shock? He was in profound cardiogenicshock. During transport, I had debated giving atropine for his bradycardia and cardiogenicshock, but was worried about making an already profoundly ischemic heart more ischemic, and chose instead to optimize preload with pressure bagging 1L NS.
When there is tachycardia, the patient is in cardiogenicshock with very poor LV function on bedside echo. We hope you can see the difference: See these cases for more examples: Syncope, Shock, AV block, Large RV, "Anterior" ST Elevation. In this case we have a crashing patient while T-wave inversion is ongoing!
Case Continued 2 days later the patient became increasingly tachycardic, hypotensive, ashen, clammy (in cardiogenicshock) and had a new murmur. The initial troponin I was 23.7 ng/ml and was falling, confirming infarction days ago. This was the 12-lead ECG. No resolution of ST elevation. The T-waves are persistently positive.
But by this time the patient went into cardiogenicshock and passed away. But the first two ECGs met Modified Sgarbossa Criteria in leads V3-4, and bedside echo found anteroseptal wall motion abnormalities corresponding with the LAD occlusion.
The patient is started on epinephrine infusion for cardiogenicshock and cardiology took the patient to the cath lab. The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria. The patient’s second troponin results at 273 ng/L and third troponin results at 320 ng/L.
An elderly man with sudden cardiogenicshock, diffuse ST depressions, and STE in aVR Literature 1. We’ve presented many variations on this theme on Dr. Smith’s Blog — with today’s case being distinguished by its discovery on abdominal exam ! 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. Left main?
I have always said that tachycardia should argue against acute MI unless there is cardiogenicshock or 2 simultaneous pathologies. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology. We showed this in a recent analysis of UTROPIA data (see abstract below).
Tachycardia is unusual in ACS unless there is cardiogenicshock or a second simultaneous pathology. To explain my opinion — I’ve added E CG # 2 to Figure-1 , which is taken from the March 12, 2018 post on Dr. Smith’s ECG blog — in which this woman in her 40s with progressively worsening dyspnea was found to have massive acute PE.
TIMI flow 0) is rare in the ED, as most either die before arrival or are recognized clinically due to cardiogenicshock. 67) Less than 3% of anterior STEMI has LM OMI, and most are recognized clinically due to cardiogenicshock. (68, Of those who do get to the ED, many present with clear STE.(65,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content