ECG Cases 48 – ECG Interpretation in Cardiac Arrest
ECG Cases
FEBRUARY 13, 2024
The post ECG Cases 48 – ECG Interpretation in Cardiac Arrest appeared first on Emergency Medicine Cases.
 Blog Cardiac Arrest STEMI
Blog Cardiac Arrest STEMI 
ECG Cases
FEBRUARY 13, 2024
The post ECG Cases 48 – ECG Interpretation in Cardiac Arrest appeared first on Emergency Medicine Cases.

Ken Grauer, MD
JUNE 14, 2024
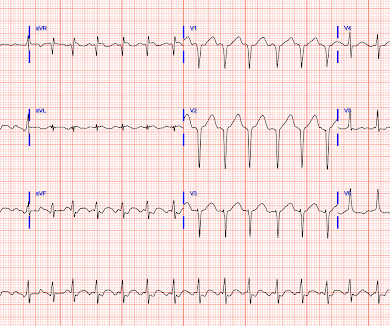
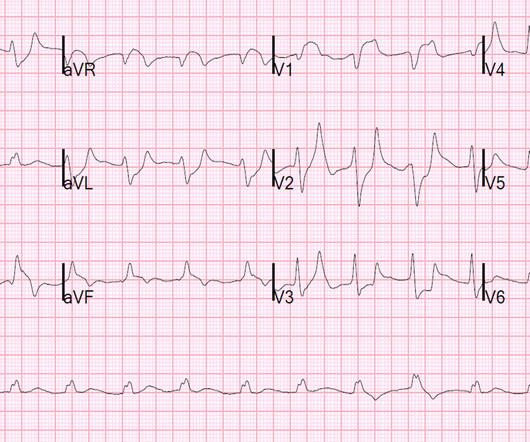
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiac arrest. Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI.

Ken Grauer, MD
FEBRUARY 3, 2024
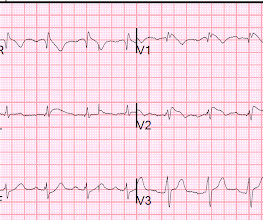
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiac arrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiac arrest. ( No CP ( C hest P ain ).
Dr. Smith's ECG Blog
JULY 9, 2024
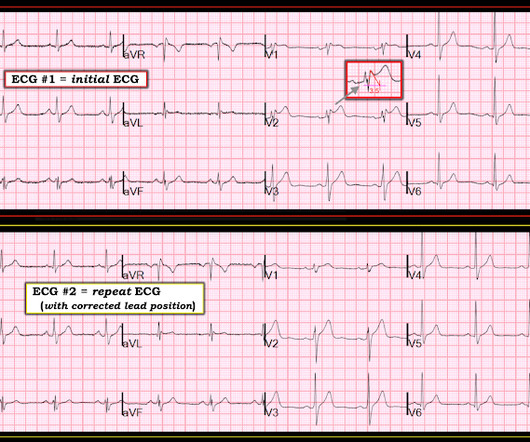
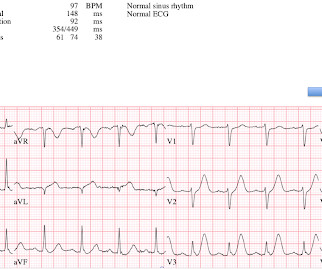
Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration. Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen. Restoration of sinus rhythm is evident in Figure-1.

Dr. Smith's ECG Blog
JULY 25, 2024
But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiac arrest, I ALWAYS wait 15 minutes after an ECG like this and record another. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR.

Ken Grauer, MD
OCTOBER 21, 2023
PEARL # 1: Although seeing an elevated Troponin would provide additional support for immediate cardiac catheterization — the clinical reality is that the initial Troponin reading will not always be elevated in patients with acute coronary occlusion ( See March 24, 2023 post in Dr. Smith's ECG Blog ).

Dr. Smith's ECG Blog
JUNE 27, 2024
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. These studies did not address OMI ECG findings!!!

Expert insights. Personalized for you.





































Let's personalize your content