This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Cardiacarrest was called and advanced life support was undertaken for this patient. The patient was given chest compressions while waiting for the cardiacarrest team to arrive. The morning before the cardiacarrest potassium was 4,3.mmol, After about 90 seconds of chest compressions she awoke.
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ).
I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiacarrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? Here is the troponin profile overnight: This is consistent with cardiacarrest without acute coronary occlusion. The QRS is extremely wide.
Cardiacarrest can cause diffuse subendocardial ischemia, usually transient (it often resolves as time goes by after ROSC). Also, anterior MI could result from 1) ACS, but also from 2) severe ischemia due to combination of a hemodynamically significant LAD stenosis + severe hypotension during cardiacarrest.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. First — Some thoughts on the post -resuscitation ECG.
Two hours later , the patient returned to this same urgent care facility with worsening chest pain, and this ECG was performed: While getting another ECG, the patient suffered cardiacarrest: After multiple defibrillations, ROSC was achieved with ongoing "STEMI". link] ] Outcome The patient emerged neurologically intact.
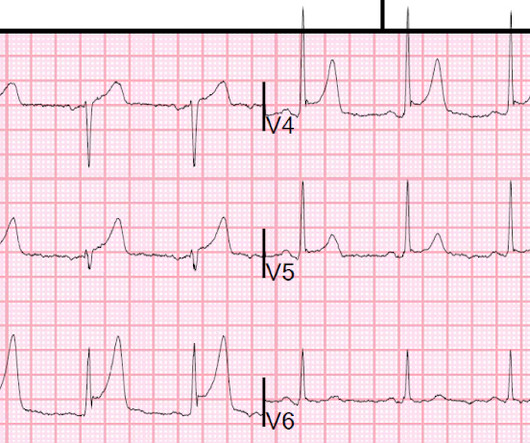
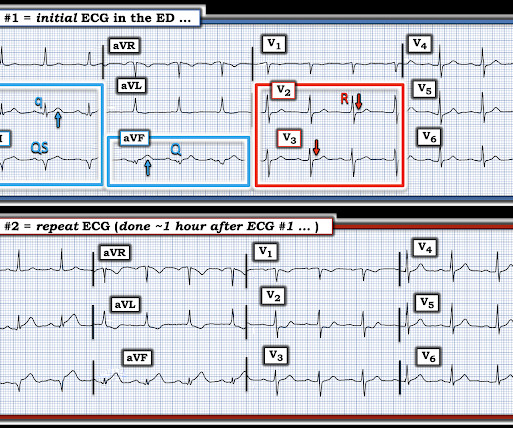
Outcome: 100% LAD Occlusion Here the Queen explains why: The dark blue tells us that she is looking especially at the QRS in V3 and the T-wave in V2 and V3. Not OMI, and we (Pendell and I) always take proportionality into account. So we taught the Queen on cases with very low voltage that were OMI.
About an hour later, he was then found on the floor in cardiacarrest in the ED. Sooner identification likely leads to better outcomes, and in this case may have allowed prevention of cardiacarrest and better long-term outcome. His initial troponin T was 15 ng/L (only two hours since pain onset).
They had had twice the rate of cardiacarrest and twice the in-hospital mortality[1] In another study of patients diagnosed with STEMI, those on dialysis experienced delayed reperfusion and double the mortality.[2] They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiacarrest. He underwent PCI and had a good outcome. Formula : There is not enough ST elevation in V2-V4 to be applying the LAD/early repol formula, but if it is applied, one gets 1.5 He was defibrillated.
But until that point, no one could have known his neurologic outcome, and the stated reason for not accepting was not worry for neurologic outcome but that the ECG did not meet STEMI criteria. The outcome measure was whether the patient ultimately had an OMI or not.
Thirty-six patients (36%) presented with cardiacarrest, and 78% (28/36) underwent emergent angiography. We’ve presented many variations on this theme on Dr. Smith’s Blog — with today’s case being distinguished by its discovery on abdominal exam ! Results Emergent angiography was performed in 80% (79/99) of patients.
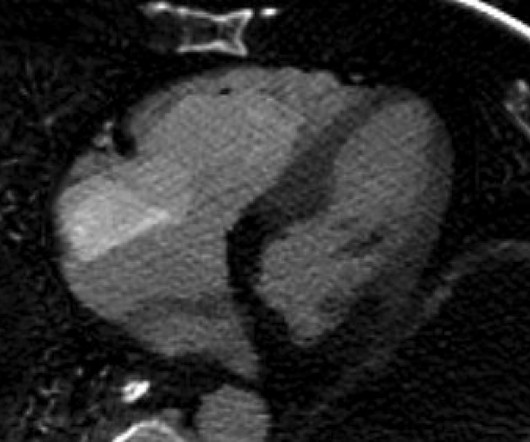
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. She was defibrillated and resuscitated. Smith: this ECG and clinical presentation is diagnostic of LAD Occlusion.
He had a previous MI with cardiacarrest 2 years prior. Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer: This is a posterolateral MI. He was clammy and looked unwell. Is this due to coronary occlusion? Some are STEMI-equivalents. This is because: 1.
Of course this is not a difficult case because one will always measure the K in such a case, but it does show that the K is markedly affecting cardiac electrical activity. Case outcome The Na was 109. This was the etiology of seizures. He was treated with hypertonic saline. Volume was down, and so repleted.
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. A reliable study would keep track of all patients with shockable arrest and analyze the ones who were not enrolled to see their outcomes. This is FAR LESS than all other studies of shockable arrest.
However, in multiple studies, even in the absence of AMI, both acute and chronic myocardial injury (as diagnosed by any elevated cTn) are powerful markers of adverse outcomes in both the short and long term. Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. 3–8 Shi et al.
Written by Pendell Meyers, with edits by Steve Smith Thanks to my attending Nic Thompson who superbly led this resuscitation We received a call that a middle aged male in cardiacarrest was 5 minutes out. He was estimated to be in his 50s, with no known PMHx. He arrived with chest compressions ongoing, intubated, and being bagged.
This blog explores how genetics influence heart health and whether mitigating these inherited risks is possible. Arrhythmias: Genetic mutations can also predispose individuals to irregular heart rhythms, such as atrial fibrillation or long QT syndrome, which may increase the risk of stroke or sudden cardiacarrest.
What is the utility of a head CT in cardiacarrest? We found intracranial hemorrhage in 2% of non-traumatic cardiacarrest patients, and in 4 others the presence of cerebral edema changed management. in Vienna found that 27 of 765 (4%) of out of hospital cardiacarrests (OHCA) were due to SAH.
The electrophysiologist is a reader of Dr. Smith's ECG Blog. Simply by correlating the history of cardiacarrest with serial ECGs recorded after the event — it became obvious that the 60% lesion on cardiac cath, despite its surprisingly good TIMI 3 flow — was indeed the "culprit" artery that had spontaneously reperfused after the event.
TCP In Transit: A case reviewing transcutaneous pacing, false electrical capture, and re-arrest. Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the first installment of a blog series showing how transcutaneous pacing (TCP) can be difficult, and how you can improve your skills. Current 85mA.
The patient stabilized and had a good outcome. If cardiacarrest from hypokalemia is imminent (i.e., As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 The mean serum potassium level was lower after resuscitation from cardiacarrest (3.6 mEq/L, from 1.9
It is highly associated with proximal LAD occlusion and bad outcomes. Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiacarrest with unrecognized STEMI, died. So this is diagnostic of proximal LAD occlusion. New RBBB + LAFB is a very bad sign.
A stent was placed, and the patient had an excellent outcome with no wall motion abnormality. Were it not for this prehospital ECG and the cardiacarrest, the diagnosis may have been significantly delayed. Angiography revealed a very tight LAD stenosis with some flow (confirming the reperfusion that we see on the ECG).
Case 1: The outcome of this case is at the far bottom. On this blog, the warning is this : It is critical to use it only when the differential is subtle LAD occlusion vs. early repol. As he was alarmed by it, he went to the patient who now was having recurrent pain, then suddenly went into cardiacarrest (ventricular fibrillation).
ECG#1 ECG#2 ECG#3 ECG#4 ECG#5 See outcomes of all 5 below, with the Queen of Hearts AI Bot interpretation. Smith: This bizarre ECG looks like a post cardiacarrest ECG with probable acidosis or hyperkalemia in addition to OMI. All of the patients presented with chest pain , and they are all in triage. What was the pH and K?
If the ventricular escape rhythm also gives out, the patient has cardiacarrest. He suffered another cardiacarrest in the ICU with ROSC after another dose of epinephrine and one round of CPR. If that limb gives out due to ischemia or another cause, the heart becomes reliant on a ventricular escape rhythm.
It is highly associated with proximal LAD occlusion or severe left main ACS and with bad outcomes. Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiacarrest with unrecognized STEMI, died. So this is diagnostic of proximal LAD occlusion. New RBBB + LAFB is a very bad sign.
Sudden cardiacarrest associated with early repolarization. Long-term outcome associated with early repolarization on electrocardiography. No one is certain what to do with this information, and it certainly does not impact emergency medicine, in which the problem remains: is it STEMI or not? N Engl J Med 2008;358(19):2016-23.
I've been working on this a long time, thought about submitting it to a journal, but decided it gets more readers on this blog. However, none of the formulas have proven to be definitively better than another and none are well correlated with outcomes or events! This article discusses correction of the QT interval for rate.
About two hours after admission, he suffered a cardiacarrest (whether it was VF/VT or PEA is not available) and expired. Like other cases on this blog who died before cath was done, I cannot prove that this patient had OMI. Could this outcome have been prevented with emergent cath? I do not accept the transfer." "It
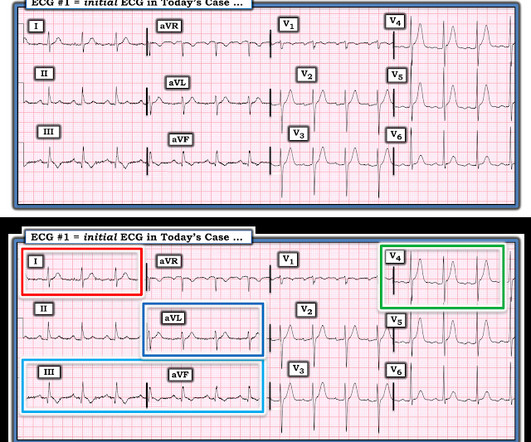
Depending on the age and sex of the patient — there may be borderline voltage for LVH ( See My Comment re LVH criteria — at the bottom of the page in the August 15, 2022 post in Dr. Smith's ECG Blog ).
Smith comment: The patient was lucky to have a cardiacarrest. By undergoing an arrest, providers became aware of his OMI which had not been noticed on his diagnostic ECG, and he thus has a chance at some myocardial salvage. Had he not had one, he would have sat in the waiting room until his entire myocardium at risk infarcted.
2] Curiously, ACLS does not include consideration of calcium in its bradycardia algorithm, which could have prevented the arrest and which along with the epi produced ROSC. HyperKalemia with CardiacArrest. Acute hyperkalemia in the emergency department: a summary from a Kidney Disease: Improving Global Outcomes conference.
The patient's long term outcome is unknown. In just 90 minutes from presentation, the patient progressed from that very subtle ECG to cardiacarrest. Dr. McLaren recently wrote an excellent blog post on a similar case. Discussion: This is a case of an initial ECG showing very subtle signs of hyperkalemia.
But it does show a strong association of better outcome with lidocaine vs. amiodarone. A retrospective 'target trial emulation' comparing amiodarone and lidocaine for adult out-of-hospital cardiacarrest resuscitation. We used propensity score matching (PSM) to investigate the association between antiarrhythmic and outcomes.
For the Queen, all 4 FPs had a culprit but the troponin was not high enough to qualify for this very strict OMI outcome definition requiring a peak hs troponin I of at least 5000 ng/L. We are lucky this patient did not have a cardiacarrest while in the Waiting Room.
They felt that the asystolic arrest suggested a different etiology of cardiacarrest. With the severe acidosis and absence of ST elevation, they felt there was more likely to be a non-cardiac etiology of his presentation. In short with a very guarded likelihood for a positive outcome.
Anyone who has been a reader of this blog understands the terrible significance of this ECG, which is diagnostic of acute proximal LAD occlusion. She survived the hospitalization, but long term outcome is not available. Plus recommendations from a 5-member panel on cardiacarrest. PMcardio digitized image.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content