This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 20-something presented after a huge verapamil overdose in cardiogenicshock. This was a very complex case and the details are too much for an ECG Blog, but suffice it to say that, s hortly thereafter, the patient had an asystolic arrest and was resuscitated. The initial K was 3.0 mEq/L and ionized calcium was 5.5
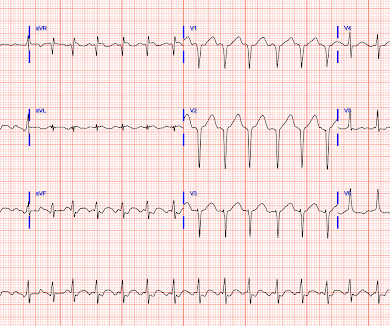
Figure B At this point, with the ECG changing from diffuse ST depression to widespread ST elevation and the patient presenting in cardiogenicshock, left main coronary artery (LMCA) occlusion is the likely diagnosis. This patient is actively dying from a left main coronary artery OMI and cardiacarrest from VT/VF or PEA is imminent!
Written by Pendell Meyers A man in his 50s was found by his family in cardiacarrest of unknown duration. Meyers and Smith in the October 15, 2022 post of Dr. Smith's ECG Blog ). His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. Restoration of sinus rhythm is evident in Figure-1.
Some patients have baseline RBBB with LAFB, but in patients with likely ACS, these are associated with severe infarction with cardiacarrest, cardiogenicshock or impending shock. Suffice it to say that, "The heart does whatever it will do when a patient is about to arrest".
About 45 minutes after the second EKG, the patient was found in cardiacarrest. A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenicshock. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest.
She arrived comatose and in cardiogenicshock and the following ECG was recorded. Before EMS arrived, she had "seizure activity" and became unresponsive. She was defibrillated successfully from ventricular fibrillation and developed a perfusing rhythm. She was intubated.
The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. As we've often emphasized on Dr. Smith's ECG Blog — it is rare in practice to see LMCA occlusion, because most such patients die before reaching the hospital. RCA — 100% proximal occlussion.
Lactate was 20, POC Cardiac US showed EF estimated at 30%, and formal echo showed EF of only 15%, and a normal RV. Assessment was severe sudden cardiogenicshock. NOTE: For those interested — I review in detail determination of the artifact “culprit extremity” in My Comment in the September 27, 2019 post of Dr. Smith’s ECG Blog.
About an hour later, he was then found on the floor in cardiacarrest in the ED. He underwent CPR and then was shocked out of VF. He was in cardiogenicshock requiring an impella for several days after cath. His initial troponin T was 15 ng/L (only two hours since pain onset). No further troponins were measured.
The patient died of cardiogenicshock within 24 hours despite mechanical circulatory support. Smith: This bizarre ECG looks like a post cardiacarrest ECG with probable acidosis or hyperkalemia in addition to OMI. This patient at cath had a large CX occlusion with a massive troponin release. Troponin T >42.000ng/L.
This pattern is essentially always accompanied by cardiogenicshock and high rates of VT/VF arrest, etc. The patient arrived to the ED in cardiogenicshock but awake. Plus recommendations from a 5-member panel on cardiacarrest. This one of the highest risk OMI patterns possible to see on an ECG.
But the lack of traditional Sgarbossa criteria is not reassuring enough for such high pretest probability (elderly patient with chest pain, out of hospital cardiacarrest and LBBB), and the Modified Sgarbossa Criteria confirms Occlusion MI in this case. But by this time the patient went into cardiogenicshock and passed away.
There was 100% proximal LAD occlusion with TIMI 0 flow, and cardiacarrest in the cath lab. Among others — See My Comment at the bottom of the page in the September 13, 2024 post of Dr. Smith's ECG Blog ). In today's case — Dr. McLaren adds a few "twists" to this clinical challenge. There is sinus tachycardia at ~100/minute.
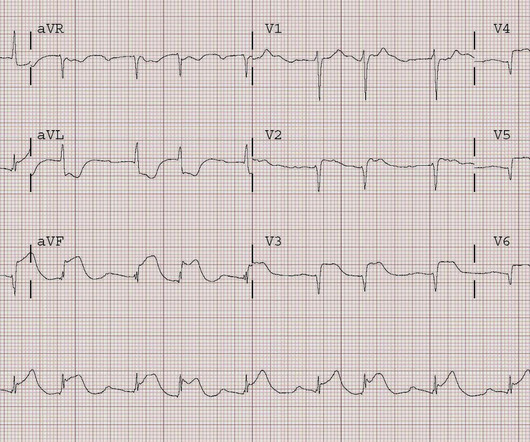
An elderly man with sudden cardiogenicshock, diffuse ST depressions, and STE in aVR Literature 1. Thirty-six patients (36%) presented with cardiacarrest, and 78% (28/36) underwent emergent angiography. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. Left main? 3-vessel disease? Knotts et al.
See our other cases with similar patters, to burn this deep into your brain files: Smith : In my experience, these cases of LAD OMI with RBBB and LAFB are either about to arrest, post-arrest, and/or in cardiogenicshock. Plus recommendations from a 5-member panel on cardiacarrest. To quote Drs.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content