This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He developed cardiacarrest shortly after the ECG in Figure-1 was recorded. As discussed in ECG Blog #231 — Bidirectional VT is a special form of VT, in which there is beat-to-beat alternation of the QRS axis. C ASE C onclusion: As noted above — today's patient developed cardiacarrest shortly after arrival in the ED.
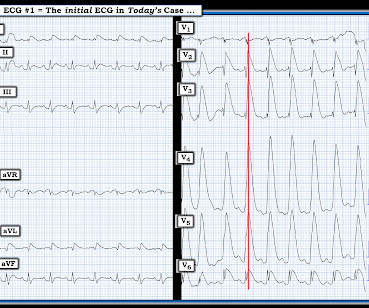
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. I i llustrate the ECG finding of T-QRS-D below in Figure-3 , which I've excerpted from My Comment in the November 14, 2019 post in Dr. Smith's ECG Blog. Should you activate the cath lab?
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiacarrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiacarrest. ( No CP ( C hest P ain ).
The H ISTORY in T oday's C ASE: The patient in today's case is a teenager who presented to the ED ( E mergency D epartment ) in cardiacarrest after electrocution. As discussed in ECG Blog #364 and ECG Blog #265 — We are looking at " Shark Fin " ST elevation! Figure-1: The initial ECG in today's case. (
The ECG in Figure-1 was obtained from an 18-year old woman — who moments before been resuscitated from out-of-hospital cardiacarrest. Does this ECG in Figure-1 provide clue(s) to the etiology of this patient's cardiacarrest? I suspected the answer resides in the reason why an 18-year woman might have a cardiacarrest.
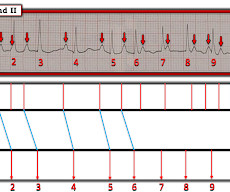
MY Approach to the Rhythm in Figure-1: As per ECG Blog #185 — I favor the P s, Q s, 3 R Approach for interpretation of the cardiac rhythm — beginning with whichever of these 5 KEY Parameters is easiest to assess for the tracing in front of me: At least in the single lead II rhythm strip seen in Figure-1 — The Q RS complex appears to be narrow.
Cardiacarrest was called and advanced life support was undertaken for this patient. The patient was given chest compressions while waiting for the cardiacarrest team to arrive. The morning before the cardiacarrest potassium was 4,3.mmol, After about 90 seconds of chest compressions she awoke.
Blood was drawn , and the patient was promptly placed in a room to be seen — but on entering, the ED physician found her unresponsive in cardiacarrest. Do you see any indication on this ECG of WHY this patient was about to arrest? Is there any indication on this ECG of WHY this patient shortly after had a cardiacarrest?
But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. See these related cases: Cardiacarrest, defibrillated, diffuse ST depression and ST Elevation in aVR.
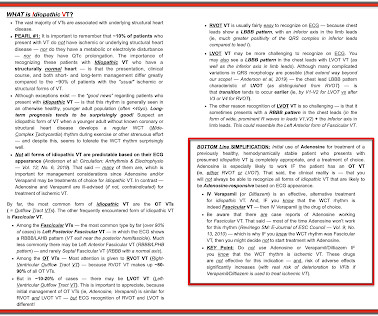
PEARL # 1: Although seeing an elevated Troponin would provide additional support for immediate cardiac catheterization — the clinical reality is that the initial Troponin reading will not always be elevated in patients with acute coronary occlusion ( See March 24, 2023 post in Dr. Smith's ECG Blog ).
Given this patient's older age — if nothing "fixable" is found, she most likely has SSS ( S ick S inus S yndrome ) and will need a pacemaker ( See ECG Blog #342 for more on SSS ). See ECG Blog #188 for review on how to read and/or draw Laddergrams ). See ECG Blog #347 for more on dual-level AV Wenckebach ).
In this CritCases blog Michael Misch takes us through a case of accidental hypothermia and cardiacarrest, reviewing the controversies in management as well as the guidelines for rewarming, the role of ECMO and the alterations to ACLS cardiacarrest medications, CPR and defibrillations.
While on telemetry monitoring he suffered cardiacarrest and was resuscitated. What ECG finding may have contributed to (or precipitated) the cardiacarrest? Learning points : Takotsubo can lead to cardiacarrest from ventricular arrhythmia. There are no clear signs of OMI. There is a prolonged QTc.
== P lease N OTE : After today — No new ECG Blog posts for 2- to -3 weeks. — I will also not be prompt in replying to emails. == All material on this ECG Blog site remains open! IF you scroll down a little on the right-hand column of this blog — You'll see a lot of icons. Figure-1: The initial ECG in today's case.
At some point ~1-2 hours after the initial ECG — the patient developed runs of VT, leading to cardiacarrest. ECG Blog #185 — Review of the P s, Q s, 3 R Approach for systematic rhythm interpretation. ECG Blog #271 — Reviews the concept of diffuse Subendocardial Ischemia. ECG Blog #316 — The patient died.
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. Coronary Angiography after CardiacArrest without ST-Segment Elevation. N Engl J Med [Internet] 2019;Available from: [link] Should all patients with shockable arrest be taken to angiography regardless of STEMI or No STEMI?
What is the cardiac rhythm shown in the long lead II rhythm strip? Figure-1: The initial ECG in today’s case — obtained from an elderly woman following successful resuscitation from cardiacarrest. ( These are reviewed in ECG Blog #343. I reviewed the concept of Echo beats in ECG Blog #239.
The Long Lead II Rhythm Strip: As always — I favor a systematic approach to rhythm interpretation, using the P s, Q s, 3 R memory aid ( See ECG Blog #185 ). As I have often emphasized — it takes a little time to get good at drawing laddergrams ( See ECG Blog #188 ). ECG Blog #108 — Reviews the concept of AIVR.
This is obviously severe hyperkalemia and the patient is near cardiacarrest. There was no IV access, so we obtained intraosseous (IO) access, but she arrested before we could give her all the calcium. Hyperkalemia and CardiacArrest Could you have prevented this young man's cardiacarrest?
See this post: How a pause can cause cardiacarrest 2. For more on Torsades de Pointes vs PMVT See My Comment in the October 18, 2023 post and the September 2, 2024 post in Dr. Smith's ECG Blog ). There is ventricular bigeminy with bizarre appearing wide T-waves See even more striking cases of this at the bottom of the post.
Sudden cardiacarrest (SCA) has had a moment in the public eye this week. Damar Hamlin's misfortune shined a public light on the grim reality that we as HCM patients live with every day: the possibility we could suffer an SCA at any moment without warning.
A woman in her 50s with dyspnea and bradycardia A patient with cardiacarrest, ROSC, and right bundle branch block (RBBB). HyperKalemia with CardiacArrest. Steve, what do you think of this ECG in this CardiacArrest Patient?" Is this just right bundle branch block?
What is the utility of a head CT in cardiacarrest? We found intracranial hemorrhage in 2% of non-traumatic cardiacarrest patients, and in 4 others the presence of cerebral edema changed management. in Vienna found that 27 of 765 (4%) of out of hospital cardiacarrests (OHCA) were due to SAH.
See our other blog posts of hypothermia and Osborn waves -- Massive Osborn Waves of Severe Hypothermia (23.6 C), with Cardiac Echo -- A Pathognomonic ECG. His temperature was brought back to normal over time in the ICU. He was extubated and had normal neurologic function. He did well and was discharged.
ST depression is common BOTH after resuscitation from cardiacarrest and during atrial fib with RVR. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiacarrest, after defibrillation, and after cardioversion. The patient was cardioverted. This was done.
I was there and said, "No, I think this is all due to severe chronic cardiomyopathy and cardiacarrest due to primary ventricular fibrillation, not due to ACS." _ Why did I say that? Here is the troponin profile overnight: This is consistent with cardiacarrest without acute coronary occlusion. The QRS is extremely wide.
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ). As a result — an ICD may need to be considered in selected cases.
Written by Pendell Meyers A man in his 50s was found by his family in cardiacarrest of unknown duration. Meyers and Smith in the October 15, 2022 post of Dr. Smith's ECG Blog ). His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. Restoration of sinus rhythm is evident in Figure-1.
Appreciation of these subtle ECG findings could have helped to avoid a cardiacarrest and its resulting permanent disability 3. Ischemia on the ECG can be very subtle and is easily missed. Accurate interpretation requires a lot of skill, practice, and experience.
This 80 year old with a history of CABG had a cardiacarrest. Now, it is true that shortly after a non-ACS cardiacarrest, there can be transient diffuse ST depression, but not ST elevation in a coronary distribution, and there should not be a wall motion abnormality. This is as clear a STEMI as you can get.
A 60-something woman presented after a witnessed cardiacarrest. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. Final Diagnosis: CardiacArrest due to Torsades from long QT of unknown etiology.
Cardiacarrest can cause diffuse subendocardial ischemia, usually transient (it often resolves as time goes by after ROSC). Also, anterior MI could result from 1) ACS, but also from 2) severe ischemia due to combination of a hemodynamically significant LAD stenosis + severe hypotension during cardiacarrest.
He had multiple cardiacarrests with ROSC regained each time. Then there is loss of pulses with continued narrow complex on the monitor ("PEA arrest") Learning Points: Sudden witnessed CardiacArrest due to ACS is almost always due to dysrhythmia. This patient arrested shortly after hospital arrival.
One hour later (labs not yet returned), here is the ECG recorded just after the team noticed a sudden wide complex with precipitous decompensation, just before cardiacarrest: Bizarre, Brady, and Broad (wide QRS). Unfortunately, this was not recognized at this time. I believe it was this point when hyperkalemia was first suspected.
Although one may have all kinds of ischemic findings as a result of cardiacarrest (rather than cause of cardiacarrest), this degree of ST elevation and HATW is all but diagnostic of acute proximal LAD occlusion. See Discussion in the June 29, 2024 post of Dr. Smith' ECG Blog ). This prompted cath lab activation.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. First — Some thoughts on the post -resuscitation ECG.
The electrophysiologist is a reader of Dr. Smith's ECG Blog. Simply by correlating the history of cardiacarrest with serial ECGs recorded after the event — it became obvious that the 60% lesion on cardiac cath, despite its surprisingly good TIMI 3 flow — was indeed the "culprit" artery that had spontaneously reperfused after the event.
NOTE: For those interested — I review in detail determination of the artifact “culprit extremity” in My Comment in the September 27, 2019 post of Dr. Smith’s ECG Blog. POINT #2: Overall QRS amplitude ( voltage ) is dramatically reduced in ECG #1. True Low Voltage is defined as a QRS amplitude of ≤5 mm in all limb leads.
TCP In Transit: A case reviewing transcutaneous pacing, false electrical capture, and re-arrest. Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the first installment of a blog series showing how transcutaneous pacing (TCP) can be difficult, and how you can improve your skills. Current 85mA.
About 45 minutes after the second EKG, the patient was found in cardiacarrest. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest. For more on Precordial Swirl — See the October 15, 2022 post in Dr. Smith's ECG Blog ).
This blog explores how genetics influence heart health and whether mitigating these inherited risks is possible. Arrhythmias: Genetic mutations can also predispose individuals to irregular heart rhythms, such as atrial fibrillation or long QT syndrome, which may increase the risk of stroke or sudden cardiacarrest.
Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management CardiacArrest. A New Seizure in a Healthy 20-something More cases of long QT not measured correctly by computer (these are all fascinating ECGs/cases): Bupropion Overdose Followed by CardiacArrest and, Later, ST Elevation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content