This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
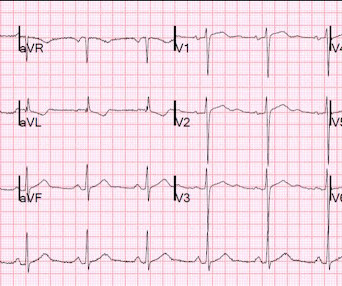
I see the following: The rhythm is sinus bradycardia at ~55-60/minute. These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ).
NOTE: As I've commented on in a number of previous blog posts — Wenckebach conduction may occur at more than a single level within the AV Node. R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #192 — The 3 Causes of AV Dissociation.
See our other countless hyperkalemia cases below: General hyperkalemia cases: A 50s year old man with lightheadedness and bradycardia Patient with Dyspnea. A woman with near-syncope, bradycardia, and hypotension What happens if you do not recognize this ECG instantly? Also: How did this happen? Is this just right bundle branch block?
There’s competing sinus bradycardia and junctional rhythm, with otherwise normal conduction, borderline right axis, normal R wave progression and voltages. While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky.
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. As discussed in ECG Blog #228 — the incidence of " Silent " MI may be as high as between 20-40% of all MIs, being especially common in older individuals. The overall ventricular response looks R egular.
There is STE in III and aVF which does not meet STEMI criteria due to insufficient STE in lead aVF. Resuscitation was initiated and this ECG was obtained: Likely AFib (irregularly irregular) with bradycardia. The cardiologists were not familiar with this and insisted that the ECG in paced rhythm could not be used to "look for a STEMI".
I will leave more detailed rhythm discussion to the illustrious Dr. Ken Grauer below, but this use of calipers shows that the rhythm interpretation is: Sinus bradycardia with a competing (most likely junctional) rhythm. For national registry purposes, this will be incorrectly classified as a STEMI.) Large STEMI are approximately 30-80.
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. EKG is pictured below: What do you think?
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. There was no evidence bradycardia leading up to the runs of PMVT ( as tends to occur with Torsades ). As we've often emphasized on Dr. Smith's ECG Blog — it is rare in practice to see LMCA occlusion, because most such patients die before reaching the hospital.
The patient has active chest pain, so if these are abnormally large T-waves This link shows 13 blog posts of Posterior Reperfusion T-waves. I did not think that the T-waves in V2 and V3 are hyperacute and I still do not--I disagree with Ken below--I think they are normal , especially in the context of bradycardia.
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 Soon afterward, the patient’s symptoms return along with lightheadedness, bradycardia, and hypotension. The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria.
His first electrocardiogram ( ECG) is given below: --Sinus bradycardia. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. If this patient was managed according to the STEMI/NSTEMI paradigm (although he would be a candidate for early invasive treatment), he would probably be taken to the cath lab hours later.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Learning Points: 1.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. He wrote most of it and I (Smith) edited.
He has been following the blog for 4 years. The emergency physician asked the advice of Dr. Reiters because of absence of STEMI criteria. This case was sent by Dr. Jean-christophe Reiters, an interventionalist in Belgium. He has now implemented the Queen of Hearts in his hospital. He wanted to share one of the first cases.
This has been discussed many times before on this blog. In-depth discussion is beyond the scope of this blog. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? The patient continued having chest pain. Do not treat AIVR. What is the rhythm? Moffat, M.
The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." Like other cases on this blog who died before cath was done, I cannot prove that this patient had OMI. The whole paradigm is literally called "STEMI" vs. "NSTEMI." Canto et al.
Three months prior to this presentation, he received a pacemaker for severe bradycardia and syncope due to sinus node dysfunction. His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”.
Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1]
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). MY Thoughts on the ECG in Figure-1: The rhythm in ECG #1 is sinus bradycardia at ~50-55/minute.
Here is his ED ECG: There is bradycardia with a junctional escape. There is an obvious inferior posterior STEMI(+) OMI. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. Results Of 149 patients with inferior STEMI , 43 (29%) had RVMI and 106 (71%) did not. What is the atrial activity?
Is it STEMI? Syncope and Bradycardia Syncope in a 20-something woman Long QT: Do not trust the computerized QT interval when the QT is long An Alcoholic Patient with Syncope Cardiac Arrest. Chest pain in high risk patient. Are these Hyperacute T-waves? What is going on here?
The Initial ECG in Today's Case: ECG #1 showed sinus bradycardia at a rate slightly under 60/minute — normal intervals — slight left axis ( about -15 degrees ) — and no chamber enlargement. Figure-1: I've labeled the 1st, 2nd and 4th tracings in today's case ( See text ).
The ECG shows sinus bradycardia but is otherwise normal. Evidence regarding intervention to non-culprit plaques is mixed and beyond the scope of this blog post. We have on many occasions in Dr. Smith's ECG Blog, highlighted the downside of indiscriminate use of morphine in patients who present with new ischemic CP ( C hest P ain ).
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chest pain: V5 and V6 sure look like a STEMI For this ECG and chest pain in the ED, the Cath lab activated. But the angiogram was clean. There was no OMI.
While undergoing a stress test as a part of the non-invasive approach, she developed chest pain and hypotension and had this ECG: There is sinus bradycardia with massive inferior ST elevation, as well as ST elevation in V1-V3, diagnostic of inferior and right ventricular (RV) STEMI.
In any case, there is bradycardia. Although most cardiac arrest from MI is due to ventricular fibrillation, some is due to high grade AV block, and so this could indeed be due to large acute STEMI. LV anterior STEMI does not give maximal ST elevation in V1. So this ECG is typical of right ventricular (RV) STEMI.
We've presented numerous examples of hyperkalemia on Dr. Smith's ECG Blog. As a reminder of why determination of the cardiac rhythm can be so challenging when there is significant hyperkalemia — I've reproduced Figure-1 from My Comment in the January 16, 2022 post in Dr. Smith's ECG Blog. The patient was treated.
My most talented blog readers are paramedics because they have to put themselves on the line every time they activate the cath lab. Trop T now very high, well into the range one sees with a STEMI; very unusual in type II MI. There is a junctional bradycardia. And they teach me a lot. Now chest pain free. What was the diagnosis?
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". Hyperkalemia causes peaked T waves and the "killer B's of hyperkalemia", including bradycardia, broad QRS complexes, blocks of the AV node and bundle branches, Brugada morphology, and otherwise bizarre morphology including sine wave. With a twist.
Without seeing the patient, my interpretation of the first ECG was: likely normal variant ST-elevation (early repolarization), with a small possibility of pericarditis, and almost no possibility of acute coronary occlusion (STEMI). and therefore highly unlikely to be STEMI.
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI.
If it is STEMI, it would have to be RBBB with STEMI. Bradycardia. But — one of the causes of Brugada Phenocopy is acute infarction — so I didn’t know how to distinguish between a preexisting Brugada-1 ECG pattern vs a Brugada ECG pattern developing as a result of acute ongoing anterior STEMI. Is it Brugada pattern?
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI. Why bradycardia? QTc is the computer measurement.
Here is his previous ECG: This was my interpretation of the first ECG: Sinus bradycardia with less than 1mm ST elevation in V4-V6, elevated compared to the previous ECG, suggestive of lateral MI. Moreover, T-wave inversion in aVL was also found to be 100% sensitive and 86% specific for inferior STEMI. mm ST depression in aVL.
Any objective, rule-based analysis of this ECG would scream "STEMI" or "OMI". And I recognized this as a STEMI mimic. Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. There are Q-waves in V4-V6, with what appear to be hyperacute T-waves.
There is sinus bradycardia with one PVC. This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI.
The computer interpreted the ECG (GE Marquette 12 SL) as: "Sinus Bradycardia. Here it is: Computer interpretation: "Sinus bradycardia. This was sent to me by a former resident from a community hospital: A middle-aged woman complained of chest pain and was seen in triage. She had a ECG recorded. Normal ECG."
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. A previous ECG from 4 years prior was normal: This looks like an anterior STEMI, but it is complicated by tachycardia (which can greatly elevate ST segments) and by the presentation which is of fever and sepsis.
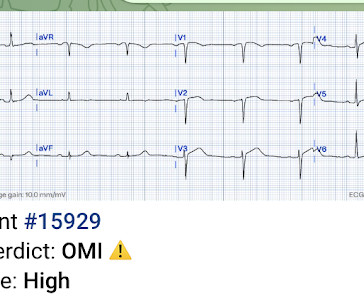
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: == MY Comment , by K EN G RAUER, MD ( 7/26 /2023 ): == As regular followers of Dr. Smith’s ECG Blog have seen — some of the best cases that we post come from tracings that Dr. Smith or Meyers see while simply checking out “tracings on the system”.
Triage physician interpretation: -sinus bradycardia -lateral ST depressions While there are lateral ST depressions (V5, V6) the deepest ST depressions are in V4. Recall that air is a poor conductor of electricity and will, therefore, generate smaller amplitudes on posterior leads (hence why STEMI criteria requires only >0.5
It does not meet STEMI criteria. Obvious STEMI(+) OMI of inferior, posterior, and lateral walls, now with likely 2nd degree heart block type 1 (Wenckebach). Learning Points: We can find OMI on ECG much sooner than STEMI criteria in many cases, and of course many OMIs never meet STEMI criteria at all. Easy for anyone.
Here are inferior leads, and aVL, magnified: A closer inspection of the inferior leads and aVL Sinus bradycardia. 3) STEMI criteria failed to identify this acute coronary occlusion, like many others. I had no history on the case and no prior ECG for comparison. What do you think? Journal of Electrocardiology 3(2):161-167; 1970.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Bicarb 20, Lactate 4.2,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content